Diabetes complications: prevention and screening

Diabetes complications
Diabetes type 2
Prevention of diabetes complications is a major aim of diabetes management and can be achieved by identification and management of people with prediabetes, early intensification of treatment to achieve optimal glycaemic control, lifestyle modifications, and regular screening for complications and their management.
- Diabetes complications are an important cause of morbidity, mortality and economic burden.
- Prevention of diabetes complications is multifactorial, including lifestyle modification, optimisation of glycaemic control, and treatment of associated cardiovascular risk factors and depression.
- The treatment algorithm for managing people with type 2 diabetes is rapidly evolving and involves early intensification of diabetes treatment regimens and use of agents that offer weight loss or neutrality in overweight and obese patients.
- Smart technology and lifestyle digital apps are being increasingly used to motivate, support and optimise management of people with diabetes.
Picture credit: © KO Studios
Prevention of diabetes complications is a major aim of diabetes management and can be achieved by identification and management of people with prediabetes, early intensification of treatment to achieve optimal glycaemic control, lifestyle modifications, and regular screening for complications and their management.
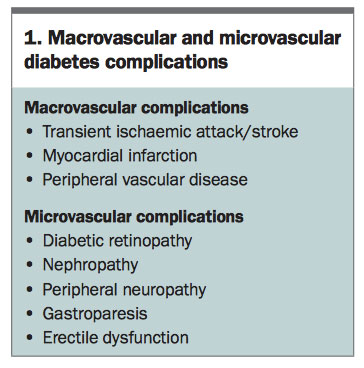
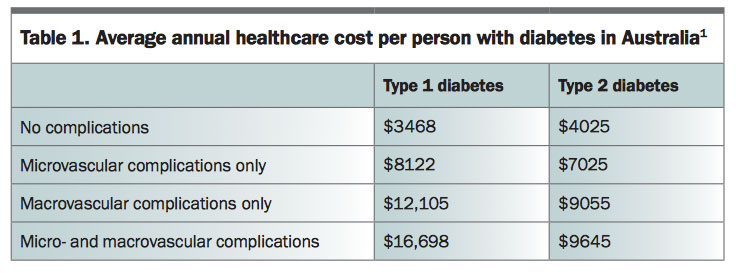
It is estimated that over 1.5 million people in Australia have diabetes, and managing this epidemic is becoming increasingly challenging.1 Diabetes is the fastest growing chronic condition in this country and with an ageing population the impact will be amplified. Diabetes complications, classified as macrovascular or microvascular (Box 1), are a major cause of associated morbidity, mortality and economic burden in our society (Table 1).1
{kind=link}
{kind=link}
Approach to preventing diabetes complications
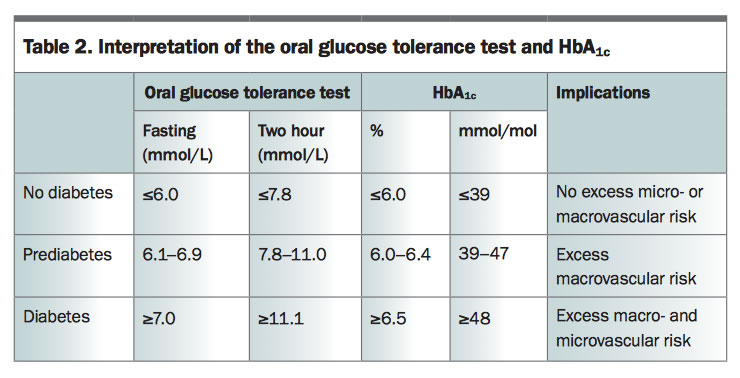
Prevention of diabetes is the holy grail of preventing diabetes complications. The Australian Type 2 Diabetes Risk Assessment Tool (see www.health.gov.au/preventionof type2diabetes) can be used to assess the risk of developing diabetes over a five-year period and identifies high-risk individuals who warrant biochemical screening.2 For people at high risk or who are symptomatic, a fasting blood glucose measurement is recommended; although oral glucose tolerance testing and HbA1c measurements can also be used (Table 2). Management of people with prediabetes should include lifestyle modification and consideration of use of adjunct pharmacological therapies such as metformin (off-label use for prediabetes) and liraglutide (TGA approved for this indication) to facilitate weight loss.3,4 Detection of prediabetes and preventing progression to diabetes clearly prevents diabetes complications.
{kind=link}
Multiple large randomised clinical trials such as the Diabetes Control and Complication Trial (DCCT) in type 1 diabetes and the United Kingdom Prospective Diabetes Study (UKPDS) in type 2 diabetes have demonstrated that intensified medication regimens are associated with a major reduction in microvascular complications.5,6 The effect on cardiovascular outcomes with such intensive regimens is less clear. The DCCT signalled a long-term benefit termed ‘the legacy effect’; however, the UKPDS did not demonstrate any significant reduction in cardiovascular events. The Action to Control Cardiovascular Risk in Diabetes (ACCORD) and The Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE) trials have also shown no reduction in cardiovascular events with near-normal glycaemic control and found that very tight glycaemic control (HbA1c <6.5% or 48 mmol/mol) may be associated with adverse outcomes due to hypoglycaemia.7 An HbA1c target of 7% (53 mmol/mol) is appropriate for most people as it achieves prevention of microvascular complications while reducing adverse events associated with hypoglycaemia. With regards to macrovascular complications, optimisation of lipid and blood pressure profiles has more significant impact than tight glycaemic control.6
Microvascular complications
Retinopathy
Diabetic retinopathy affects approximately 15% of patients with diabetes and is the leading cause of visual impairment in people of working age in Australia.8,9 The risk of retinopathy increases with HbA1c levels above target, with a longer duration of diabetes and in the presence of other microvascular complications, especially nephropathy. Pregnancy and rapid establishment of normoglycaemia in a patient with previous suboptimal glycaemic control can temporarily exacerbate retinopathy.10,11
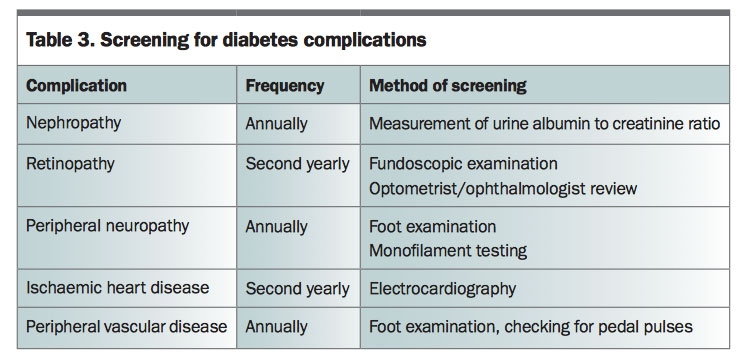
Screening for retinopathy and early referral of the patient to an ophthalmologist, if appropriate, can prevent vision loss. Unfortunately, currently up to 30% of patients with diabetes are not screened appropriately according to guidelines; reminder systems to alert the clinician and patient should be used to minimise this. Testing for visual acuity (with correction) together with fundoscopic examination by an optometrist or ophthalmologist is recommended second yearly or annually if other risk factors are present (Table 3).12 Use of nonmydriatic retinal cameras to document and monitor progress is now covered by Medicare.
{kind=link}
Treatment of retinopathy may involve laser photocoagulation and intravitreal injections with antivascular endothelial growth factors. Two prospective studies, Fenofibrate Intervention and Event Lowering in Diabetes (FIELD) and ACCORD Eye, revealed reductions in progression of retinopathy with intensive medical management to optimise glycaemia and dyslipidaemia.13,14 Hypertension can accelerate and worsen retinopathy and pharmacological treatment should be used to achieve a target blood pressure of 130/80 mmHg.
Nephropathy
The most common cause of end-stage renal disease (ESRD) in Australia is diabetic nephropathy, which accounts for over 30% of all patients requiring dialysis. Certain groups such as Aboriginal Australians, New Zealand Maoris and South Pacific Islanders are particularly susceptible and may progress quickly to ESRD. Concomitant hypertension also accelerates this progression.15
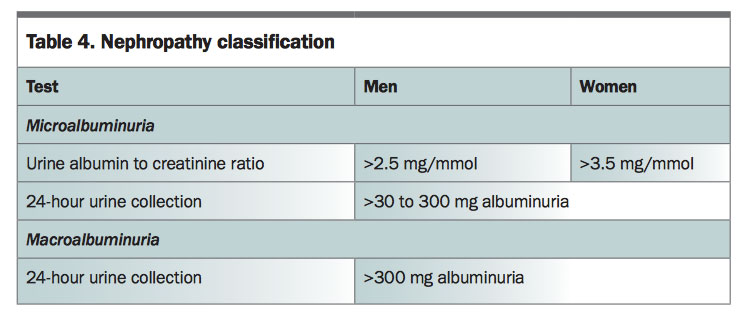
Screening for nephropathy usually involves measuring the albumin to creatinine ratio in a spot urine sample to detect microalbuminuria, which obviates the need for a 24 hour urinary collection (Table 3). The presence of microalbuminuria identifies patients who are at an increased risk of progressing to macroalbuminuria, and once macroalbuminuria is established there is an increased risk of progression to ESRD over the next 10 years (Table 4).
{kind=link}
The presence of chronic kidney disease (CKD) limits the use of several oral hypoglycaemic agents that are renally excreted. Current guidelines recommend that metformin can be safely used at a maximum dose of 1 g daily if the estimated glomerular filtration rate (eGFR) is 30 to 60 mL/min/1.73 m2 or more; however, it should be ceased once eGFR is less than 30 mL/min/1.73 m2.16 Short-acting sulfonylureas such as gliclazide may be used in people with CKD but long-acting agents such as glibenclamide are associated with a high risk of hypoglycaemia and should be avoided. Certain dipeptidyl peptidase-4 (DPP-4) inhibitors such as linagliptin are safe to use, whereas others such as sitagliptin, saxagliptin and vildagliptin require dose adjustments and should be used with caution. Cardiovascular risk optimisation, including treatment of hypertension and dyslipidaemia, is essential because microalbuminuria and CKD are independent risk factors for cardiovascular disease. The sodium-glucose cotransporter-2 (SGLT-2) inhibitor empagliflozin was recently shown to have renoprotective effects in patients with type 2 diabetes at high risk of cardiovascular events and can be used in those with an eGFR of 45 mL/min/1.73 m2 or more.17
Angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs) are the preferred initial antihypertensive therapy to reduce proteinuria, with the addition of calcium channel blockers if blood pressure targets are not met.
Neuropathy
Peripheral neuropathy can predispose to diabetic foot infections and lead to loss of limbs. Patients at high risk of diabetic foot infections include those with a history of foot ulcers or with more than two risk factors (e.g. neuropathy, peripheral arterial disease or foot deformity). These patients should be enrolled in a foot protection program and have regular podiatry follow up.18 Patients at low risk should have a foot examination yearly, assessing sensation, skin condition, pressure areas, bony architecture and pedal pulses, and should be educated about appropriate footwear.18
The presence of peripheral vascular disease impedes blood flow and wound healing therefore treatment of hypertension and dyslipidaemia, together with smoking cessation, is imperative. A recently published study demonstrated that statins may protect against lower limb amputation in patients with diabetes.19
Evidence of acute infection such as fever, cellulitis or purulent discharge from a diabetic foot ulcer requires urgent inpatient treatment with intravenous antibiotics and vascular assessment for consideration of surgical debridement. Unfortunately, studies such as UKPDS and ADVANCE have not demonstrated improvement or reduction in progression of peripheral neuropathy with tight glycaemic control.
Autonomic dysfunction
Autonomic dysfunction may be difficult to identify but can have significant impact on a patient’s function and wellbeing. Gastroparesis is a debilitating complication leading to early satiety and gastrointestinal symptoms such as abdominal pain and bloating. Insulin management can be challenging in these patients who often need to eat small frequent meals.
Erectile dysfunction, postural hypotension, sinus tachycardia and electrocardiographic evidence of previous silent myocardial infarction are signs of potential underlying autonomic neuropathy. Acute coronary syndrome may present atypically (with reduced or absence of chest pain), and the presence of autonomic neuropathy is known to increase the risk of sudden cardiac death.
Management of autonomic dysfunction includes optimising glycaemic control to prevent further progression of neuropathy, optimisation of cardiovascular risk factors and early specialist referral.
Macrovascular complications
Macrovascular complications are the major cause of morbidity and mortality in people with type 2 diabetes. Absolute cardiovascular disease risk calculators (www.cvdcheck.org.au) can be used to assess the risk of a macrovascular event in the next five years in people aged 45 years or older. People with diabetes who are at high risk should be treated with blood pressure-lowering and lipid-lowering agents unless contraindicated or clinically inappropriate.20 The role of aspirin in primary prevention of acute coronary syndromes in people with diabetes remains controversial.21
Recently three cardiovascular safety trials of glucose-lowering medications have demonstrated a benefit in cardiovascular mortality in patients with type 2 diabetes at moderate to high risk of cardiovascular disease. The first of these trials, Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients (EMPA-REG OUTCOME), demonstrated a 38% relative risk reduction in death from cardiovascular causes with use of empagliflozin (an SGLT-2 inhibitor), and also beneficial effects on hospitalisation for heart failure, weight loss and systolic blood pressure compared with placebo.22 The Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results (LEADER) trial investigated the role of liraglutide, a once-daily glucagon- like peptide-1 (GLP-1) analogue, in patients with type 2 diabetes at high risk of cardiovascular disease.23 A 22% relative risk reduction in death from cardiovascular causes compared with placebo was found.23More recently, the preapproval Trial to Evaluate Cardiovascular and Other Long-term Outcomes with Semaglutide in Subjects with Type 2 Diabetes (SUSTAIN-6) demonstrated a 26% relative risk reduction in death from cardiovascular causes with use of semaglutide, a once weekly GLP-1 analogue currently in development, with most benefit arising from a reduction in nonfatal stroke.24 In contrast, the Evaluation of Lixisenatide in Acute Coronary Syndrome (ELIXA) trial demonstrated no evidence of cardiovascular protection with use of the once-daily GLP-1 agonist lixisenatide in patients with recent acute coronary syndrome.25
Three trials investigating the DPP-4 inhibitors saxagliptin (Saxagliptin Assessment of Vascular Outcomes Recorded in Patients with Diabetes Mellitus; SAVOR TIMI-53), alogliptin (Examination of Cardiovascular Outcomes: Alogliptin versus Standard of Care in Patients with Type 2 Diabetes Mellitus and Acute Coronary Syndrome; EXAMINE) and sitagliptin (The Trial to Evaluate Cardiovascular Outcomes after Treatment with Sitagliptin; TECOS) did not demonstrate superiority with regards to cardiovascular protection. However, they met primary composite cardiovascular safety end-points, albeit with some unresolved issues such as increased risk of hypoglycaemia and the adverse impact of saxagliptin on hospitalisation for heart failure, which does not appear to be a class effect.26
So how do we incorporate this evidence into clinically appropriate practice? As there are few head-to-head trials guiding the choice of agent management decisions should be individualised based on treatment responses and tolerability within the framework of the PBS. All the agents that have shown benefit in cardiovascular mortality should be considered in high risk patients. The Australian Diabetes Society’s evidence-based interactive program available online can assist in the navigation of the evolving treatment plan (t2d.diabetessociety.com.au).
Optimising cardiovascular risk factors
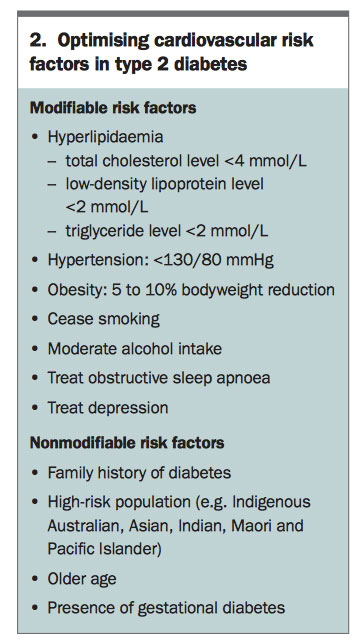
Optimisation of cardiovascular risk factors in patients with type 2 diabetes is essential to reduce macrovascular complications (Box 2). Patients with diabetes who are over 60 years of age or have documented microalbuminuria have high absolute risk of cardiovascular disease and should be commenced on lipid-lowering and blood pressure-lowering therapy unless contraindicated or clinically inappropriate.20 For low-risk patients who are unable to achieve lipid targets with lifestyle modification, statins are the preferred agent to achieve a low-density lipoprotein level of less than 2.5 mmol/L for primary prevention. For secondary prevention, intensive lipid lowering with use of the highest tolerated dose of statin is indicated. Blood pressure management should involve commencement of an ACE inhibitor or ARB to achieve a target of less than 130/80 mmHg.27 If the blood pressure target remains unmet despite the highest tolerated dose of an ACE inhibitor or ARB, then a calcium channel blocker such as amlodipine should be added to the regimen.
{kind=link}
Smoking significantly increases risk of macrovascular complications in people with type 1 or type 2 diabetes, and cessation should be strongly encouraged. Depression can affect multiple domains of diabetes care, including adherence to medication and diet and willingness to participate in exercise and lifestyle changes, as well as independently increasing risk of cardiovascular disease. Recognition and treatment of depression in the primary care setting is an essential component of an individualised diabetes care plan.
Screening for macrovascular complications is currently not recommended; however, comprehensive risk assessment for cardiovascular disease would include taking a thorough history for symptoms suggestive of cardiac ischaemia such as exertional chest pain and dyspnoea, clinical examination and electrocardiography. If concerning symptoms or signs are present, patients should be referred promptly for cardiac stress testing to investigate underlying ischaemic heart disease.20
Managing acute diabetes complications
A hyperosmolar hyperglycaemic state can occur in people with type 2 diabetes, often with a triggering event such as infection, myocardial infarction or nonadherence to medications. Inpatient management involves intravenous hydration, slow reduction of blood glucose level and treatment of the precipitant. Diabetic ketoacidosis occurs more often in people with type 1 diabetes but is seen in those with type 2 diabetes with a long history of diabetes and very low endogenous insulin production. Euglycaemic diabetic ketoacidosis can occur with use of SGLT-2 inhibitors, especially in the context of reduced oral intake, intercurrent illness and alcohol intake. It is imperative patients cease these agents if such clinical situation arises, and clinicians should check for ketosis and acidosis.28
Acute hyperglycaemia in a person with well-controlled diabetes should alert the clinician to potential aggravators such as glucocorticoid use and subclinical infections such as candidiasis. Hypoglycaemia can be particularly dangerous in patients with underlying significant coronary artery disease or epilepsy. Hypoglycaemic awareness may be blunted in patients with a long duration of type 1 diabetes, autonomic neuropathy and concomitant treatment with beta blockers. For patients with frequent hypoglycaemic episodes, treatment should be adjusted to lessen the risk of hypoglycaemia and HbA1c targets relaxed.
Intensification of diabetes regimen starts early
The benefits of intensified glycaemic control appear to be greatest in the early stages of diabetes management.6,29 Therefore, uptitration of oral hypoglycaemic agents and injectables should not be delayed in the primary care setting, and further modification to ensure targets are reached should be continued throughout the entire treatment period.
Overweight and obese people with diabetes require tailored management to optimise glycaemic control and use of agents that can exacerbate weight gain, such as sulfonylureas and insulin, should ideally be reduced. Practice has rapidly evolved to use agents that promote weight loss or neutrality, such as metformin, DPP-4 inhibitors (sitagliptin, linagliptin, saxagliptin, vildagliptin), SGLT-2 inhibitors (empagliflozin, dapagliflozin) and GLP-1 analogues (exenatide, liraglutide). Weight loss surgery should also be considered in obese patients with significant insulin resistance.30
Smart technology for diabetes
Regular monitoring of blood glucose levels assists in optimisation of diabetes treatment regimens, especially for people taking insulin. Many of the available blood glucose monitoring devices have memory and download features to review readings, calculators to dose correctional and prandial insulin based on carbohydrate intake and talking features for vision-impaired patients. The new FreeStyle Libre Flash Glucose Monitoring System is an interstitial glucose monitoring system that has revolutionised diabetes monitoring, especially for people with type 1 diabetes, by allowing the detection of trends and tracking patterns without the need for calibration with finger-prick capillary blood glucose measurement. The soon to become available Guardian Connect by Medtronic can be useful for people with type 1 diabetes who engage in frequent or high-intensity exercise, have variable routines (e.g. shift work) or have labile glycaemic control to help clinicians fine tune their insulin regimens.
Insulin pumps are sophisticated and effective treatment for patients with type 1 diabetes, enabling precise titration of basal insulin rates and frequent correction for hyperglycaemia. Development is under way of a closed loop system using a continuous glucose monitoring device that communicates with an insulin pump equipped with algorithms that alter insulin delivery to prevent excursions from normoglycaemia.
Multidisciplinary care
Diabetes educators are an integral part of the team to update and educate patients on all aspects of care, including availability and use of smart meters and technology to optimise glycaemic control. Dietitians are essential for patient education on carbohydrate counting, portion control and making healthy dietary choices to manage dyslipidaemia. In patients with type 1 diabetes, titration of rapid-acting insulin according to carbohydrate intake prevents prandial glycaemic excursions.
For overweight and obese people with type 2 diabetes, restriction of dietary intake with very low-calorie diets usually requires adjustments of oral hypoglycaemic agents and insulin to avoid hypoglycaemia. Overweight and obese patients with physical restrictions may benefit from referral to an exercise physiologist who can tailor programs to suit individual needs.
Psychologists can help patients develop positive and sustained lifestyle changes and provide strategies for those with low mood and motivation.
Lifestyle modification in the digital age
Diet and exercise are essential components of diabetes management regimens. Mobile phone applications such as CalorieKing and Easy Diet Diary can help patients to calorie count and keep track of their dietary intake. Exercise applications such as inbuilt phone pedometers and Runkeeper can be used to calculate daily step count. Activity trackers such as FitBit, Garmin and Apple watches can also calculate steps taken plus have other capabilities such as calculating distance travelled and calories burned.
It is important to note that exercise can lead to hyperglycaemia and hypoglycaemia, and may require adjustments to insulin regimens. People who engage in regular exercise may also need to downtitrate their medication because of improved glycaemic control. Resources to promote healthy diet and lifestyle changes are essential and novel strategies such as personal group training and fitness programs, support from online communities, training for fun runs and community events can also be used to motivate patients.
Conclusion
Complications secondary to diabetes are a major contributor to morbidity, mortality and economic burden in our healthcare system. Prevention of diabetes complications is the main aim of diabetes management and can be achieved by identification and management of people with prediabetes, early intensification of treatment to achieve optimal glycaemic targets, lifestyle modifications and regular screening for complications.ET
References
- Shaw J, Tanamas S. Diabetes: the silent pandemic and its impact on Australia. Diabetes Aust 2012: 1-5 en L, Magliano DJ, Balkau B, Colagiuri S, Zimmet PJ. AUSDRISK: an Australian type 2 diabetes risk assessment tool based on demographic, lifestyle and simple anthropometric measures. Med J Aust 2010; 192: 197-202. Pi-Sunyer X, Astrup A, Fujioka K, et al. A randomized, controlled trial of 3.0 mg of liraglutide in weight management. N Engl J Med 2015; 373: 11-22.
- Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 2002; 346: 393-403.
- The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993; 329: 977-986.
- UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes. Lancet 1998; 352: 837-853.
- Dluhy RG, McMahon GT. Intensive glycemic control in the ACCORD and ADVANCE trials. N Engl J Med 2008; 358: 2630-2633.
- Tapp, RJ, Shaw JE, Harper CA, et al. The prevalence of and factors associated with diabetic retinopathy in the Australian population. Diabetes Care 2003; 26: 1731-1737.
- Australian Institute of Health and Welfare. 2008 Diabetes: Australian facts 2008. Diabetes series no. 8 Cat. no. CVD 40. Canberra: AIHW.
- Heath V. Diabetes: Progression of diabetic retinopathy found to be a potential risk during pregnancy. Nat Rev Endocrinol 2010; 6: 354.
- Brinchmann-Hansen OK, Dahl-Jorgensen K, Sandvik L, Hanssen KF. Blood glucose concentrations and progression of diabetic retinopathy: the seven year results of the Oslo study. BMJ 1992; 304: 19-22.
- National Health and Medical Research Council. Guidelines for management of diabetic retinopathy. Canberra: Australian Diabetes Society for the Department of Health and Ageing; 2008.
- Keech AC, Mitchell P, Summanen PA, et al. Effect of fenofibrate on the need for laser treatment for diabetic retinopathy (FIELD study): a randomised controlled trial. Lancet 2007; 370: 1687-1697.
- ACCORD Study Group; ACCORD Eye Study Group. Effects of medical therapies on retinopathy progression in type 2 diabetes. New Engl J Med 2010; 363: 233-244.
- Van Buren PN, Toto R. Hypertension in diabetic nephropathy: epidemiology, mechanisms, and management. Adv Chronic Kidney Dis 2011; 18: 28-41.
- Lipska KJ, Bailey CJ, Inzucchi SE. Use of metformin in the setting of mild-to-moderate renal insufficiency. Diabetes Care 2011; 34: 1431-1437.
- Wanner C, Inzucchi SE, Lachin JM et al. EMPA-REG OUTCOME Investigators. Empagliflozin and progression of kidney disease in type 2 diabetes. N Engl J Med 2016; 375: 323-334.
- National evidence-based guideline on prevention, identification and management of foot complications in diabetes (Part of the Guidelines on management of type 2 diabetes). Canberra: Commonwealth of Australia, 2011.
- Yang T-L, Lin L-Y, Huang C-C, et al. Association of statin use and reduced risk of lower-extremity amputation among patients with diabetes: a nationwide population-based cohort observation. Diabetes Care 2016; 39: e54–e55.
- National Vascular Disease Prevention Alliance. Guidelines for the management of absolute cardiovascular disease risk. 2012. Available online at: https://www.heartfoundation.org.au/images/uploads/publications/Absolute-CVD-Risk-Full-Guidelines.pdf (accessed March 2017).
- Ogawa H, Nakayama M, Morimoto T, et al. Low-dose aspirin for primary prevention of atherosclerotic events in patients with type 2 diabetes: a randomized controlled trial. JAMA 2008; 300: 2134-2141.
- Zinman B, Wanner C, Lachin JM, et al; EMPA-REG OUTCOME Investigators. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 2015; 373: 2117-2128.
- Marso SP, Daniels GH, Brown-Frandsen K, et al; LEADER Trial Investigators. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2016; 375: 311-322.
- Marso SP, Bain SC, Consoli A, Eliaschewitz FG, et al; SUSTAIN-6 Investigators. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med 2016; 375: 1834-1844.
- Pfeffer MA, Claggett B, Diaz R, et al; ELIXA Investigators. Lixisenatide in patients with type 2 diabetes and acute coronary syndrome. N Engl J Med 2015; 373: 2247-2257.
- Ghosal S, Sinha B. Gliptins and cardiovascular outcomes: a comparative and critical analysis after TECOS. J Diabetes Res 2016; 2016: 1643496.
- The Royal Australian College of General Practitioners. General practice management of type 2 diabetes – 2014–15. Melbourne: RACGP; 2014.
- Rosenstock J, Ferrannini E. Euglycemic diabetic ketoacidosis: a predictable, detectable, and preventable safety concern with SGLT-2 inhibitors. Diabetes Care 2015; 38: 1638-1642.
- Kerr D, Partridge H, Knott J, Thomas PW. HbA(1c) 3 months after diagnosis predicts premature mortality in patients with new onset type 2 diabetes. Diabet Med 2011; 28: 1520-1524.
- Schauer PR, Bhatt DL, Kirwan JP, Wolski K, Brethauer SA; STAMPEDE Investigators. Bariatric surgery versus intensive medical therapy for diabetes – 3-year outcomes. N Engl J Med 2014; 370: 2002-2013.
COMPETING INTERESTS: Dr Kumar: None.
Dr Colman has received clinical trial funding from NovoNordisk, Eli Lilly, Janssen, Boehringer Ingelheim, Medtronic and Lexicon.