Cushing's syndrome as a cause of secondary hypertension

Cushing's syndrome
Hypertension
A 37-year-old woman presents to her GP with weight gain and hypertension. Her diagnosis of Cushing’s syndrome is discussed.
Julie’s past medical history is signicant only for a previous left metatarsal fracture after a similar injury. Her blood pressure readings about 12 months ago were less than 125/80mmHg. There is a family history of hypertension, it being diagnosed in her mother at the age of 64 years. She takes a combined oral contraceptive pill (COCP) and no other regular medications. She has gained 10 kg over the past two years, despite an acceptable diet and regular gym attendance. She lives with her husband and two children, who also attend your practice. She is a nonsmoker, drinks alcohol only occasionally and works as a schoolteacher.
What is your initial impression?
Answer: Julie presents with nonspecific symptoms, but her blood pressure reading taken in the emergency department is significantly elevated and requires further attention. The differential diagnoses for an elevated blood pressure are broad and include essential hypertension and secondary hypertension from renal, endocrine or medication-related causes. The headache history could be related to her elevated blood pressure, and further history taking would assist in delineating between primary causes of headache (migraine, tension, cluster) and secondary causes (intracranial infection, haemorrhage, tumour, temporal arteritis, medication overuse). The chronic nature of the headache makes infection or acute haemorrhage unlikely. She also has a history of two metatarsal fractures sustained with minimal trauma, raising the possibility of osteoporosis.
How would you direct your examination?
Answer: A thorough physical examination is required.
Her abdomen is soft, with no palpable masses or organomegaly, but there are prominent abdominal striae with a purple tinge. There is acne present on the face and upper chest. She appears mildly hirsute with small amounts of terminal hair on the upper lip and chin and light hair growth in the sideburn area. There is no facial plethora.
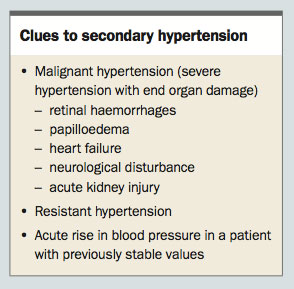
What clinical features suggest secondary causes of hypertension?
Answer: Clinical clues suggestive of secondary hypertension are listed in the Box, and can occur in combination or isolation. Your suspicion of this condition is raised with Julie as she has acute, significant elevation of a previously normal blood pressure.
{kind=link}
{kind=link}
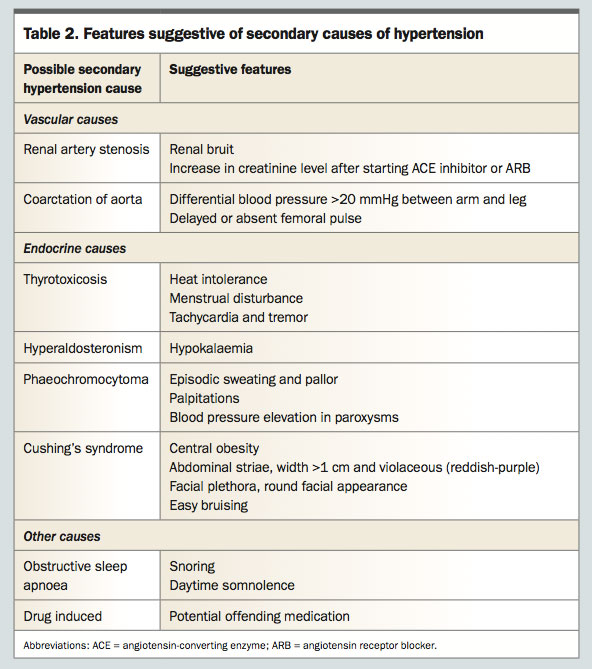
What are the possible causes of secondary hypertension and what is the most likely cause in this patient?
Answer: Secondary hypertension should be considered in young patients or those with resistant hypertension, especially as there is potential to correct the underlying aetiology. It should be remembered that renovascular hypertension is the most common cause of secondary hypertension. Symptoms and examination findings suggestive of the various secondary causes of hypertension are listed in Table 2, and include hypokalaemia (hyperaldosteronism), episodic sweating and pallor (phaeochromotocytoma) and renal bruits (renal artery stenosis). An approach to the investigation of suspected secondary hypertension is given in the flowchart.1 First-line investigations include testing renal function, thyroid function, aldosterone to renin ratio, renal artery imaging and screening for obstructive sleep apnoea with a sleep study. However, if clinical clues are suggestive of a specific aetiology, investigations can be directed accordingly.
{kind=link}
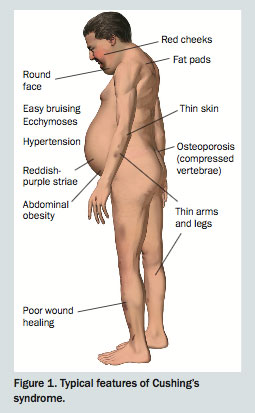
In Julie’s case, the history of weight gain and acne and the presence of abdominal striae are suggestive of Cushing’s syndrome. Abdominal striae are a nonspecific finding; those suspicious of Cushing’s syndrome are violaceous (reddish-purple) in colour and more than 1 cm in width (Figure 1).2
{kind=link}
Many drugs can affect blood pressure, including the oestrogen component of the oral contraceptive pill. Usually the blood pressure elevation in women taking the pill is mild, but occasionally it can be malignant.3 If it is true drug-induced hypertension, a trial off the offending medication for several weeks will lead to a return to baseline blood pressure levels within months.
How would you manage the blood pressure in this setting, and what are some red flags that indicate the need for acute assessment in the emergency department?
Answer: An elevated blood pressure reading should be monitored across several office visits, and white-coat syndrome considered. The white-coat hypertension effect can occur in patients with apparently resistant hypertension, and ambulatory blood pressure monitoring (ABPM) can be used to determine this.4 In true hypertension, the average daytime blood pressure reading on ABPM is above 140/90 mmHg, and the average sleeping blood pressure is above 125/75 mmHg.5
Malignant hypertension is a severe blood pressure elevation associated with acute end organ damage, and patients require emergency department referral.
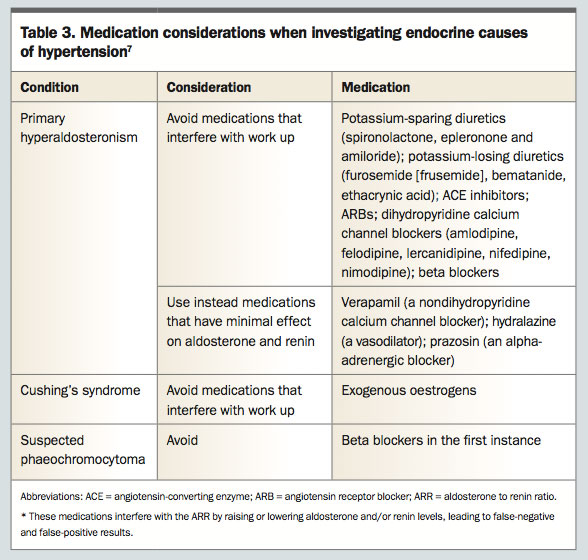
If endocrine causes of hypertension are suspected, care must be taken when choosing an antihypertensive medication as many interfere with the interpretation of aldosterone and renin measurements in investigative testing, leading to a delay in diagnosis (Table 3).6 Some medications require cessation for up to six weeks before testing. This is especially relevant in the work up for hyperaldosteronism.
{kind=link}
On the contrary, particular antihypertensives can exacerbate blood pressure in certain pathologies. This particularly applies to the use of beta blockers in phaeochromocytoma that can precipitate a catecholamine crisis. Blockade of peripheral beta-adrenergic receptors can lead to unopposed alpha-adrenergic stimulation leading to further elevation in blood pressure.7 If a phaeochromocytoma is suspected, then safe alternatives include calcium channel blockers and alpha blockers. The main priority is to avoid beta blockade in the first instance.
Ultimately the timely treatment of acute severe elevation in blood pressure is important. An endocrinologist can assist in subsequently adjusting antihypertensive medications in patients requiring further work up.
What is Cushing’s syndrome and what are the typical features?
Answer: Cushing’s syndrome is a collection of signs and symptoms that result from a state of chronic hypercortisolism. The elevated levels of cortisol can be due to either endogenous overproduction of cortisol (endogenous Cushing’s syndrome) or exogenously administered glucocorticoids (iatrogenic [or exogenous or drug-related] Cushing’s syndrome). Cushing’s syndrome due to exogenous glucocorticoid excess (e.g. prednisolone) is most common. The condition can manifest with varied sequelae, including metabolic (glucose intolerance, obesity, sleep apnoea), dermatological (acne, striae, skin atrophy and easy bruising, supraclavicular fat pads and round face), reproductive (menstrual irregularities, signs of androgen excess), cardiovascular (hypertension, increased cardiovascular risk), musculoskeletal (proximal weakness, bone loss) and neuropsychological (depression, emotional lability) disorders.1 The typical features of a person with Cushing’s syndrome are shown in Figure 1.
Patients with prolonged adrenocorticotrophic hormone (ACTH)-dependent Cushing’s syndrome may display generalised hyperpigmentation. This is secondary to ACTH binding to melanocyte-stimulating hormone receptors. Cortisol does not contribute to pigmentation.
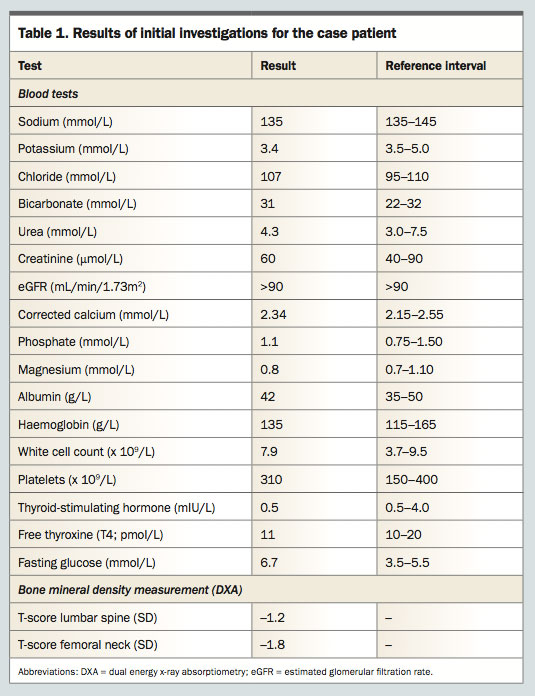
The main suggestive features of Cushing’s syndrome in Julie are her raised fasting glucose level, hypertension, history of weight gain, acne and minimal trauma fractures.
Who should be tested for Cushing’s syndrome?
Answer: Many of the features of Cushing’s syndrome are nonspecific. The syndrome is most suggested if multiple symptoms develop and worsen simultaneously, but no single feature is necessary for diagnosis. The most common manifestations of glucose intolerance, obesity and hypertension are also common in individuals without hypercortisolism. Hence the diagnosis can be difficult to make, and must be confirmed by biochemical testing. Before testing, however, a careful history should be taken to exclude exogenous glucocorticoid exposure.8
Screening for Cushing’s syndrome should be conducted in patients with:
- unusual findings for their age (osteoporosis or hypertension in young adults)
- progressive features of Cushing’s syndrome
- unexplained severe features at any age (osteoporosis or hypertension)
- adrenal incidentalomas.
Julie has a borderline low serum potassium level. How could this be explained?
Answer: Occasionally Cushing’s syndrome can lead to hypokalaemia. At high serum concentrations, cortisol can exhibit mineralocorticoid activity, leading to potassium loss.9 However, if hypertension presents in combination with hypokalaemia without cushingoid features, it would be appropriate to consider a more common secondary cause of hypertension, namely Conn’s syndrome (primary hyperaldosteronism). Hypokalaemia in Conn’s syndrome results from excess aldosterone secretion by adrenal adenoma(s) or bilateral adrenal hyperplasia. Conn’s syndrome is more common than Cushing’s syndrome, and is screened for by the determination of the plasma aldosterone to renin ratio (ARR) in the absence of interfering medications. It is reasonable to consider both pathologies in Julie’s case.
You suspect hypercortisolism in Julie. What further investigations should be performed in a patient with suspected hypercortisolism?
Answer: The diagnosis of hypercortisolism is established if there are two abnormal results for investigations for Cushing’s syndrome.8 These investigations include:
- 24-hour urine free cortisol (UFC)
- 1 mg overnight dexamethasone suppression test (DST)
- midnight salivary cortisol measurement.
These tests have different sensitivities and specificities, and often repeat investigations are required.
Multiple first-line tests are recommended if the index of suspicion of Cushing’s syndrome is high. Testing should be performed on multiple occasions as cortisol secretion can follow a cyclical pattern in states of normal cortisol secretion and hypercortisolism, and an abnormally high level may be missed on a single screening test. An abnormal result should prompt referral to an endocrinologist, who will arrange further testing, assist in excluding pseudo-Cushing’s syndrome and conduct further investigation to determine the cause of Cushing’s syndrome.8
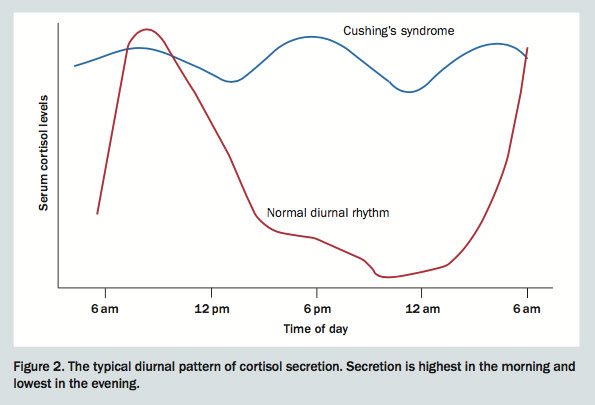
Note that an elevated random morning cortisol level is NOT indicative of cortisol excess. As cortisol secretion carries a diurnal pattern, cortisol is at its physiological peak in the morning and hence a raised morning cortisol level, in isolation, is not an indication of cortisol excess (Figure 2). At midnight, cortisol secretion is at its physiological trough, and hence a high midnight cortisol level (as in a midnight salivary cortisol measurement) is an indication of cortisol excess, and also of the loss of diurnal variation seen in states of abnormal endogenous cortisol excess.
{kind=link}
It is also appropriate to test Julie’s plasma free metanephrines and aldosterone and renin levels at this point as part of the work up for secondary causes of hypertension.
- ARR, 10 (reference interval, <70)
- 24-hour UFC, 2090 nmol/L (<330 nmol/L)
- midnight salivary cortisol, 16 nmol/L (0.2–3.2 nmol/L)
- plasma free metanephrines, 0.3 nmol/L (<0.4 nmol/L).
Julie is taking a COCP. What effect could this have on your investigation interpretation?
Answer: Oestrogen-containing medications such as COCPs or hormone therapy can lead to false elevations in cortisol levels. This is secondary to increased levels of cortisol-binding globulin.10 The dexamethasone suppression test should not be used in patients taking exogenous oestrogens; alternatively, oestrogens can be ceased at least six weeks before testing. Urinary free cortisol measurements are not affected by changes in cortisol-binding globulin.
What is the difference between pseudo-Cushing’s syndrome and Cushing’s syndrome?
Answer: Cushing’s syndrome may result from ACTH-dependent causes (i.e. ACTH-secreting pituitary adenomas [known as ‘Cushing’s disease’] and ectopic ACTH secretion by nonpituitary tumours) and ACTH-independent causes (i.e. adrenocortical adenomas and carcinomas, and exogenous glucocorticoids) of hypercortisolism.
In pseudo-Cushing’s syndrome, the hypercortisolism is secondary to other factors but the clinical and biochemical features can be similar. Pseudo-Cushing’s syndrome can occur in obesity, chronic alcohol intake, major illness and major psychological stress.8 It should be excluded when evaluating patients for Cushing’s syndrome. Note that Julie’s level of alcohol intake is not sufficient to cause pseudo-Cushing’s syndrome.
Investigation for a pituitary adenoma as an underlying cause of excess ACTH secretion is best performed by a pituitary MRI. Large pituitary adenomas may also be visualised on cerebral CT scanning.
Her endocrinologist arranged a pituitary MRI, which identified a 5 mm pituitary adenoma. To confirm a pituitary source of excess ACTH secretion, a specialised invasive test was conducted, namely inferior petrosal sinus sampling. This demonstrated a characteristic gradient with significantly higher ACTH level in blood sampled from the inferior petrosal sinus (i.e. pituitary venous drainage) compared with the peripheral circulation. She was therefore diagnosed with ACTH-dependent Cushing’s syndrome (Cushing’s disease) and referred to a neurosurgeon. She underwent transsphenoidal resection of her pituitary adenoma.
Postoperatively, she requires hydrocortisone replacement and is considered to be in remission of her Cushing’s disease. She has lost 5 kg of weight, and her energy levels have drastically improved. Pleasingly, her blood pressure has normalised. Over time, with gradual recovery of pituitary function, the hydrocortisone will be weaned. She will continue to have lifelong pituitary hormone monitoring, including monitoring for recurrence of Cushing’s disease.
References
- Viera AJ, Neutze DM. Diagnosis of secondary hypertension: an age-based approach. Am Fam Physician 2010; 82: 1471-1478.
- Ross EJ, Linch DC. Cushing’s syndrome – killing disease: discriminatory value of signs and symptoms aiding early diagnosis. Lancet 1982; 320: 646-649.
- Chasan-Taber L, Willett WC, Manson JE, et al. Prospective study of oral contraceptives and hypertension among women in the United States. Circulation 1996; 94: 483-489.
- Muxfeldt ES, Bloch KV, Nogueira Ada R, Salles GF. True resistant hypertension: is it possible to be recognized in the office? Am J Hypertens 2005; 18: 1534-1540.
- Head GA, Mihailidou AS, Duggan KA, et al. Definition of ambulatory blood pressure targets for diagnosis and treatment of hypertension in relation to clinic blood pressure: prospective cohort study. BMJ 2010; 340: c1104.
- Funder JW, Carey RM, Fardella C, et al. Case detection, diagnosis, and treatment of patients with primary aldosteronism: an endocrine society clinical practice guideline. J Clin Endocrinol Metab 2008; 93: 3266-3281.
- Lenders JW, Duh QY, Eisenhofer G, et al. Pheochromocytoma and paraganglioma: an endocrine society clinical practice guideline. J Clin Endocrinol Metab 2014; 99: 1915-1942.
- Nieman LK, Biller BM, Findling JW, et al. The diagnosis of Cushing’s syndrome: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 2008; 93: 1526-1540.
- Christy NP, Laragh JH. Pathogenesis of hypokalemic alkalosis in Cushing’s syndrome. N Engl J Med 1961; 265: 1083-1088.
- Burke CW. The effect of oral contraceptives on cortisol metabolism. J Clin Path 1969; s1-3: 11-18.