Managing glucose during exercise in type 1 diabetes

Diabetes type 1
Sports fitness
Education on exercise and diabetes self-management is important to enable people with type 1 diabetes to exercise safely, and particularly to reduce the risk of exercise-induced hypoglycaemia.
- Fear of hypoglycaemia and development of unstable blood glucose levels are some barriers to exercise in people with type 1 diabetes.
- Exercise can increase the risk of hypoglycaemia during the exercise session and also for up to 48 hours afterwards, including overnight hypoglycaemia.
- Glucose response to exercise varies with type, duration and intensity of exercise, as well as other factors such as circulating insulin levels, food intake (timing and composition) and exercise conditions.
- Glucose management strategies such as insulin dose reduction and carbohydrate consumption around exercise need to be tested, then individualised based on glucose trends.
Picture credit: © Fertnig/adobe.com Model used for illustrative purposes only.
Regular exercise is recommended for people with type 1 diabetes. Exercise has been shown to improve fitness, lipid profile, endothelial function, insulin resistance and quality of life in people with type 1 diabetes.1 Observational studies have found an association with physical activity and reduced cardiovascular disease and mortality in people with type 1 diabetes.1-3 Despite these known benefits, many people with type 1 diabetes do not undertake the recommended levels of physical activity. In adults with type 1 diabetes, major barriers to physical activity include fear of hypoglycaemia and unstable blood glucose levels, including hyperglycaemia.4 Implementing strategies to minimise the risk of exercise-induced hypoglycaemia in particular are important so that people with type 1 diabetes can safely participate in exercise.
Exercise recommendations
For adults with either type 1 or type 2 diabetes, a minimum of 150 minutes of moderate-intensity aerobic physical activity is recommended per week, with no more than two consecutive days without exercise.5,6 An alternative option is 75 minutes per week of vigorous-intensity aerobic physical activity, or an equivalent combination of moderate and vigorous-intensity aerobic physical activity, again spread across the week. In addition, reduction of sedentary time is encouraged, particularly breaking up periods of prolonged sitting exceeding 90 minutes.
The recommendation for all children, including children with diabetes, is to encourage 60 minutes of physical activity every day, involving vigorous-intensity aerobic activity, muscle strengthening activities and bone-strengthening activities on at least three days per week.5
Some people with diabetes complications (such as severe cardiac disease, proliferative diabetic retinopathy, peripheral neuropathy, autonomic neuropathy) may require further individualised assessment for a tailored safe exercise prescription.
Acute effects of exercise on glucose
Overall, exercise most commonly results in an acute decrease in blood glucose concentration.7 However, different exercise types, intensities and duration can have different effects on glucose in people with type 1 diabetes. Continuous moderate-intensity aerobic exercise is more likely to cause a greater drop in blood glucose levels compared with resistance exercise.8 High-intensity interval training, which involves brief periods of high-intensity exercise including anaerobic exercise with short intervening periods of rest, results in a less pronounced drop in blood glucose levels than during continuous moderate-intensity aerobic exercise.8 In contrast, continuous high-intensity exercise can cause hyperglycaemia in people with type 1 diabetes due to the catecholamine-mediated increase in endogenous glucose production.9,10
Exercise-induced hypoglycaemia occurs in people with type 1 diabetes because of relative hyperinsulinaemia from insulin treatment. Exercise can cause enhanced insulin mobilisation due to increased blood flow to subcutaneous depots in exercised regions. This elevated insulin level during exercise opposes the effect of glucagon on endogenous glucose production from the liver, and can also accentuate glucose uptake in muscle, both contributing to the fall in glucose levels and increasing the risk of hypoglycaemia.9
Delayed effects of exercise on glucose
Postexercise late-onset hypoglycaemia, including overnight hypoglycaemia, can occur in people with type 1 diabetes, particularly when the exercise is more intense or prolonged than typical for the person.11 There is a significant risk of delayed hypoglycaemia occurring many hours after an exercise session, with the highest risk between six and 15 hours after exercise (but can occur up to 31 hours postexercise).11,12
Physiological mechanisms for postexercise late-onset hypoglycaemia include extraction of glucose from the circulation to replenish muscle and liver glycogen stores, enhanced insulin sensitivity and reduced counter-regulatory hormone response to hypoglycaemia.11
Factors affecting glucose response to exercise
In addition to exercise characteristics including type, intensity, timing in day and duration, there are many other factors that influence the glucose response to exercise, including:
- food intake (timing and composition)
- pre-exercise glucose levels
- recent hypoglycaemia (this can blunt the usual counter-regulatory hormone responses to exercise and thus increase exercise-induced hypoglycaemia)13
- circulating insulin levels
- emotional state (emotions, such as the excitement associated with a major competitive sporting event, can increase
- catecholamine levels resulting in a rise in blood glucose levels)14
- intercurrent illness
- physiological state changes (such as diurnal hormone
- variations, menstrual cycle and pregnancy)
- environmental conditions (e.g. heat, cold, humidity, altitude).
Strategies to manage glucose during exercise in type 1 diabetes
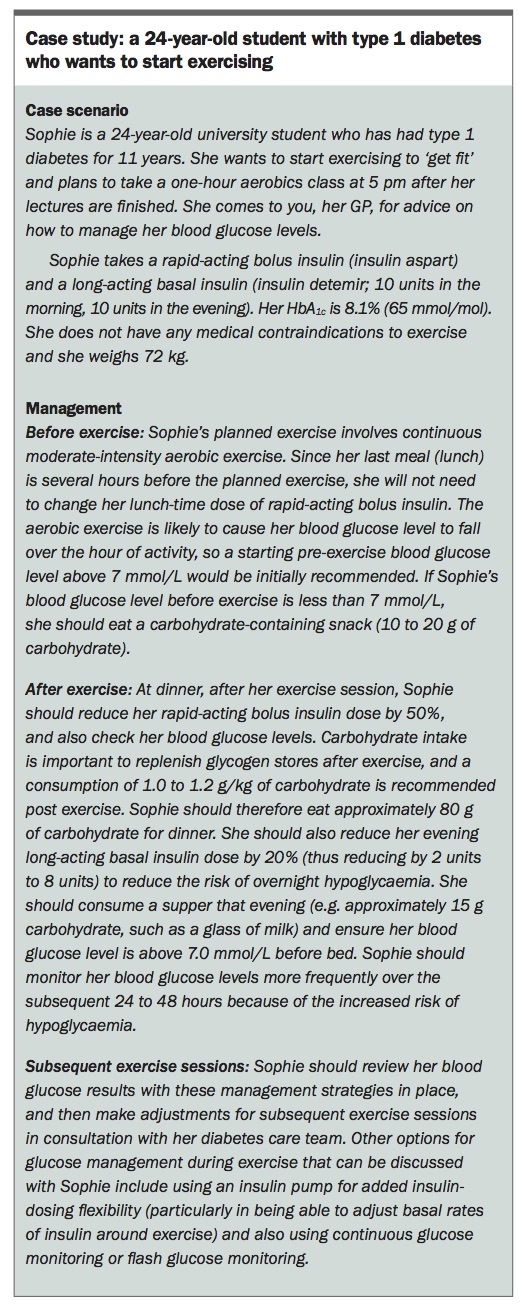
Glucose management during exercise is centred on appropriate glucose monitoring, adjustments to basal and bolus insulin, and consumption of carbohydrates.6 Almost all forms of exercise lasting greater than 30 minutes will require some alteration in food or insulin to prevent hypoglycaemia.14 Glucose responses are generally more predictable in people who have greater cardiovascular fitness, have better long-term glycaemic control and undertake exercise as a regular routine daily or second daily.15
General principles to managing glucose control around exercise are provided as a starting point for clinical care, and can be tailored to suit individual glucose responses (see case study in the Box). Personal exercise goals should be considered when tailoring glucose management strategies.6 For example, people striving for weight loss may opt for reducing insulin doses rather than consuming extra carbohydrates with the aim of preventing hypoglycaemia, whereas athletes may opt for specific additional nutritional supplementation especially with rapid-acting carbohydrate, with the goal of maximising exercise performance.
{kind=link}
When exercising, a person with type 1 diabetes needs to have glucose monitoring equipment as well as readily available snacks for treatment of hypoglycaemia. They should also ideally carry diabetes identification. Examples of food items useful for immediate hypoglycaemia treatment (containing 15 grams of fast-acting carbohydrate) include three to four glucose tablets, seven jellybeans, a half cup of juice or regular soft drink, 1 tablespoon of honey or 1 tablespoon of sugar. Examples of snacks containing 15 grams of long-acting carbohydrate include an apple, a banana, a slice of bread, a cup of yoghurt, a cup of milk and a muesli bar.
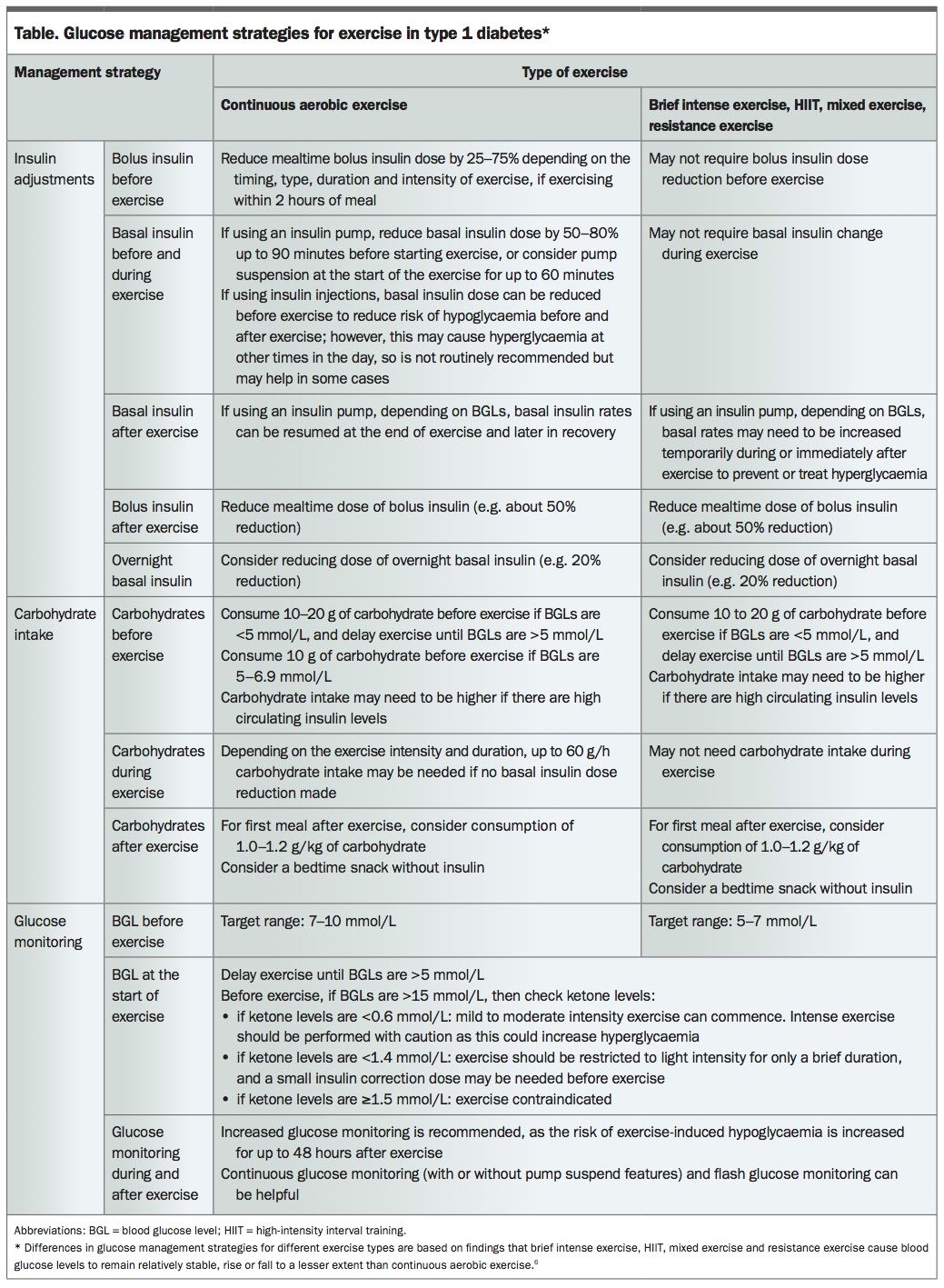
Glucose management strategies for exercise, including alterations in insulin dosing and carbohydrate intake, are shown in the Table. There is significant variability in glucose response to exercise between people, and the recommendations should be used as a guideline starting point for subsequent individualised management based on glucose monitoring results. In general, these strategies take into account the typically greater fall in glucose levels caused by continuous aerobic exercise. This is in contrast to other forms of exercise (such as high-intensity interval training and resistance exercise) in which glucose levels can fall to a smaller extent, remain stable or even rise. All forms of exercise can increase the risk of delayed overnight hypoglycaemia.
{kind=link}
In addition to the recommendations in the Table, other glucose management considerations during exercise for people with type 1 diabetes include:
- using an insulin pump, which may be more easily adjusted for exercise, particularly when exercise is not preplanned, compared with insulin injections. By reducing basal rates on an insulin pump around exercise, the amount of extra
- carbohydrates consumed to manage glucose levels may be reduced; however, insulin pumps may not be suitable for all people and there are additional challenges for contact sports (such as martial arts, football)
- avoiding alcohol when exercising, as it inhibits gluconeogenesis and can increase risk of hypoglycaemia
- maintaining adequate hydration, which may include use of sugar-free fluids
- keeping records of exercise (type, duration and intensity),
- insulin dose, food intake and glucose results, which can help tailor individualised glucose management strategies for exercise
- performing resistance exercise in a session before aerobic
- exercise, which can help reduce postexercise hypoglycaemia compared with aerobic exercise alone
- performing a short 10-second maximal sprint immediately before or immediately after aerobic exercise, which may reduce hypoglycaemia risk during early recovery16,17
- exercising in the early morning, which may help to reduce nocturnal hypoglycaemia
- using technology such as continuous glucose monitoring and low-glucose suspend features on insulin pumps, which may help with glycaemic control and particularly to avoid
- exercise-related hypoglycaemia. Although current sensors are reasonably accurate, inaccuracies may be increased during times of rapid glucose change
- considering a therapeutic use exemption for insulin in
- athletes competing in high-level sport (www.asada.gov.au/therapeutic-use-exemption).
Much of the above information is included in the online patient educational tool ExT1D.com.au, which has recently been clinically researched to show a reduction in hypoglycaemic events related to exercise in people with type 1 diabetes who use this website.18
Conclusion
The challenges in glucose management with exercise may be one of the reasons why many people with type 1 diabetes do not do enough exercise. Diabetes self-management education on exercise is important to enable people with type 1 diabetes to exercise safely, and in particular to reduce the risk of exercise-induced hypoglycaemia. A starting guide is provided in this article, emphasising that personalising strategies in optimising glucose care around exercise are required in each person with type 1 diabetes. ET