Prediabetes: early identification key to halting progression

Diabetes type 2
Diabetes medicines
People with prediabetes will benefit from early identification using diabetes risk scores for the general population, and then further blood testing for those who are identified as being at high risk of developing type 2 diabetes. A lifestyle intervention program should be commenced in people with prediabetes and pharmacological agents considered to prevent or slow the transition to diabetes.
- Prediabetes is a high-risk state for developing type 2 diabetes and is also associated with a higher cardiovascular disease risk.
- Early detection and treatment of prediabetes can delay the onset and reduce the risk of developing diabetes.
- A two-stepped approach based on diabetes risk scores for the general population and further blood tests for those who are identified as high risk is recommended for prediabetes screening.
- If prediabetes is detected, lifestyle changes should be commenced to prevent or slow the transition to diabetes. Aggressive cardiovascular risk reduction should be instituted.
- To improve diabetes prevention, a multifaceted approach that targets physicians’ understanding and compliance
with guidelines, as well as interventions to diminish
patient barriers to diabetes prevention is necessary.
Picture credit: © WavebreakmediaMicro/stock.adobe.com Models used for illustrative purposes only
Diabetes, particularly type 2 diabetes, is a global epidemic. In 2014, 422 million adults were estimated to have diabetes worldwide,1 and this is expected to increase to 629 million by 2045.2 In Australia, the prevalence of diabetes has more than doubled during the past two decades and the number of people with diabetes is projected to reach two million in 2025.3,4
Prevention of type 2 diabetes is a major global public health challenge. Individuals who have raised blood glucose levels, but are below the threshold for diabetes, are defined as having prediabetes (impaired glucose tolerance [IGT] and/or impaired fasting glucose [IFG]). Without intervention, 15 to 30% of people with prediabetes will develop type 2 diabetes within five years.5,6 In individuals without diagnosed diabetes, the two-hour postprandial glucose level on oral glucose tolerance testing (OGTT) and fasting blood glucose level are significant predictors of all-cause and cardiovascular disease mortality.7,8
Emerging evidence from observational studies and randomised controlled trials has clearly shown that people at the prediabetes stage will benefit from early identification followed by intensive lifestyle intervention and pharmacological treatment to delay the onset and reduce the risk of developing diabetes.9-13 Furthermore, their elevated cardiovascular risk merits a more aggressive approach to blood pressure and lipid management. However, most patients with prediabetes are not identified, let alone treated. This article focuses on the approaches to the early identification of people with prediabetes and strategies and barriers for diabetes prevention.
Prediabetes screening
Most people with prediabetes are unaware that they have the condition. The infrequency of screening for prediabetes may be due in part to lack of a screening strategy suitable for the general population. The most sensitive way to screen is to use the OGTT, but it is invasive, time consuming, expensive and impractical at the population level. Hence, a simple method for identifying high-risk individuals would be an advantage. To be practical on a large scale, such a method needs to use readily available information and not require blood testing. Such screening tools can then be used by the general public directly, as well as by healthcare professionals. Once individuals who are at high risk have been identified using such a tool, they can progress to more definitive blood testing to identify those with prediabetes or diabetes.
Preliminary noninvasive assessment
A large number of simple screening tools have been described. They essentially use information on well-known risk factors for type 2 diabetes to produce a score indicating the risk that the individual will progress to type 2 diabetes over the subsequent few years. There is often a perceived need to develop ethnic-specific or country-specific tools. However, we recently reported that the need for ethnic-specific or country-specific tools may have been overestimated, and that it may be more important to develop or identify tools that use measurements that are clearly described and have high reproducibility in both research and clinical settings.14
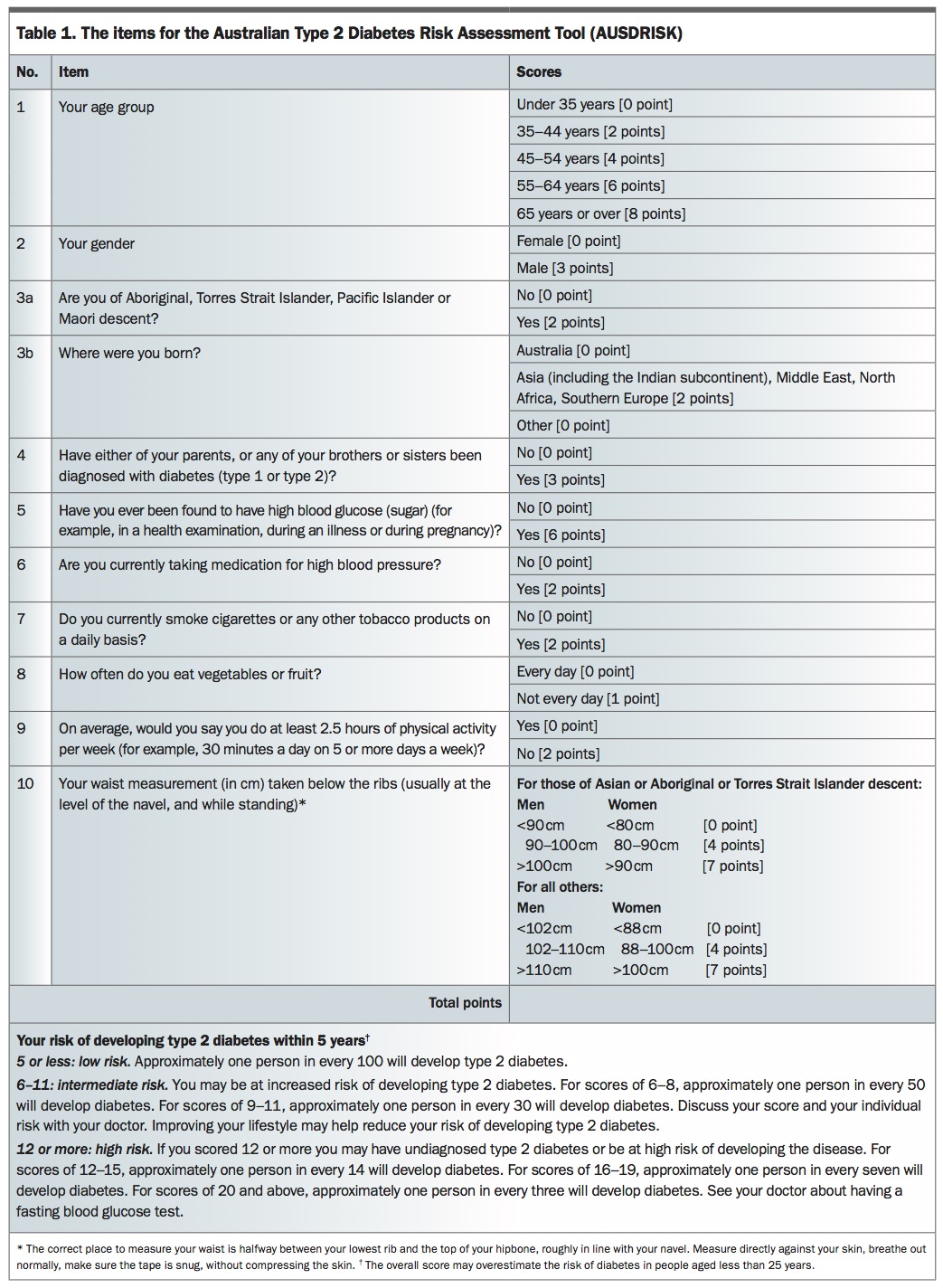
The Australian Type 2 Diabetes Risk Assessment Tool (AUSDRISK) is a simple and noninvasive diabetes risk score that can be well understood and used by lay people, and the results calculated without any laboratory tests.15 The AUSDRISK was developed using Australian data to identify adults at high risk of type 2 diabetes who might benefit from interventions to prevent or delay its onset, and was validated in three other Australian studies.16-18 AUSDRISK is based on nine risk factors including age, sex, ethnicity, parental history of diabetes, history of high blood glucose level, use of antihypertensive medications, smoking, physical inactivity and waist circumference. It has been converted into a points-based, patient-friendly questionnaire (Table 1 and see https://static.diabetesaustralia.com.au/s/fileassets/diabetes-australia/6d252140-1ff0-47b2-a83f-3cc3db348131.pdf) and there is also an online interactive version (www.baker.edu.au/health-hub/diabetes-risk-assessment). Individuals with an AUSDRISK score of 12 or more (corresponding to 12.7% probability of developing diabetes during five years of follow up) are identified as being at high risk, and should proceed to diagnostic blood testing. AUSDRISK can be used in any individual aged 25 years or above, but is not necessary in those who are manifestly at high risk (e.g. previous gestational diabetes, known prediabetes, a prior cardiovascular event or polycystic ovary syndrome), all of whom should proceed directly to blood testing.
{kind=link}
Using this simple and valid questionnaire as a preliminary screening method, followed with more invasive and accurate diagnosis with blood testing, can be a cost-effective and practical method to screen for prediabetes. AUSDRISK can be used by allied healthcare professionals or by patients themselves, for example in the doctor’s waiting room.
Diagnostic testing
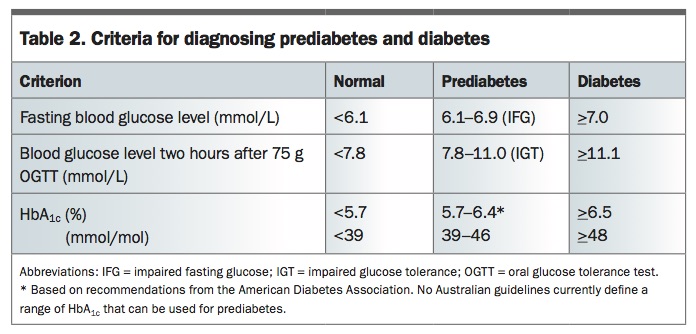
The best validated diagnostic tests for prediabetes are the two-hour postprandial glucose level on OGTT and the fasting blood glucose level. IGT is defined as a blood glucose level two hours after a 75 g oral glucose load of 7.8 to 11.0 mmol/L and a fasting blood glucose level in the nondiabetic range. IFG is defined as a fasting blood glucose level of 6.1 to 6.9 mmol/L (Table 2). These are the most studied prediabetes states. HbA1c has in recent years also attracted attention as a means of diagnosing prediabetes. No Australian guidelines currently define a range of HbA1c level that can be used for prediabetes, but the American Diabetes Association recommends using 5.7 to 6.4% (39 to 46 mmol/mol) and the World Health Organization simply notes that as HbA1c level gets closer to the 6.5% (48 mmol/mol) that defines diabetes, the risk of future diabetes rises.
{kind=link}
These three potential ways of diagnosing prediabetes (IGT, IFG and elevated HbA1c level) do not necessarily identify the same individuals. Furthermore, nearly all of the evidence for the prevention of progression to diabetes is in people with IGT, and not in those with other forms of prediabetes. Nevertheless, all people identified as having prediabetes by any method should be considered for lifestyle intervention. This should be most intensively pursued in people with IGT, as the risk of progression to type 2 diabetes is high and the evidence for benefit is strong. For people prepared to consider an intensive lifestyle change program, the OGTT is a valuable diagnostic test, whereas for other people, either measurement of the fasting blood glucose or HbA1c level will provide adequate information.
Strategies for diabetes prevention
Lifestyle modification should be the cornerstone of treatment for people with prediabetes, owing to its safety and effectiveness. Components of lifestyle intervention include modification to nutrition, increase in exercise, weight reduction and tobacco cessation. The 2002 Diabetes Prevention Program study demonstrated that lifestyle interventions in people with prediabetes significantly reduced the risk of progression to type 2 diabetes by up to 58% compared with placebo.9 These landmark findings were confirmed by several other large randomised controlled trials and the benefits have lasted up to 10 years in longitudinal observational studies.19-22
Lifestyle interventions to reduce the risk of progression to diabetes
In the American College of Endocrinology and the American Association of Clinical Endocrinologists Consensus Statement published in 2008, a program of regular moderate-intensity physical activity for 30 to 60 minutes daily, at least five days per week, is recommended and a diet that includes calorie restriction, increased fibre intake and possible limitations in carbohydrate intake is advised.23
In addition to increasing moderate-intensity physical activity, reducing and regularly interrupting prolonged sitting time has the potential to improve cardiometabolic health.24 Although a definitive threshold of sedentary behaviour reduction that will promote health improvements is unclear at present, evidence to date suggests that reductions of at least 60 minutes per day may be required for clinical benefit in the prevention of type 2 diabetes.25,26
Resistance training is increasingly recognised as an important treatment component for people with prediabetes and is particularly beneficial for older people with prediabetes given the loss of lean body mass with advancing age. Regular resistance training engagement (one to two sessions per week) is associated with lower odds of impaired glucose metabolism and all-cause mortality, and improved physical functioning.27-29
How to translate lifestyle studies into clinical practice
The main challenge is how best to deliver and achieve engagement with these interventions and how to sustain lifestyle change. One-on-one sessions with a dietitian or other qualified healthcare professional are unlikely to be feasible in clinical practice because of the large numbers of people who need such services, and the limited staff and resources available. In 2013, a review synthesised evidence from 17 translational studies to assess the impact of lifestyle interventions delivered outside large randomised trials, and found that group-based interventions could yield significant weight loss (with the expectation of reductions in the risk of type 2 diabetes), and that changes were sustained over several years.30 Thus, the beneficial effects of intensive lifestyle interventions that have been proven in randomised controlled trials can be replicated in community settings where resources are more limited and samples less selective than in the trial environment.
Pharmacological agents to prevent the development of diabetes
The use of metformin or acarbose has been shown in randomised multicentre interventional trials to reduce the progression of prediabetes to diabetes.9,31 However, the effect is smaller than that of intensive lifestyle intervention and after their discontinuation the incidence of diabetes increases. Furthermore, long-term benefit of such drugs on cardiovascular outcomes in people with prediabetes has not been demonstrated. Several clinical trials, including findings from the Diabetes Reduction Assessment with Ramipril and
Rosiglitazone Medication trial, Diabetes Prevention Program and Actos Now for Prevention of Diabetes trial, have shown that use of thiazolidinediones decreases the likelihood of progression from prediabetes to diabetes.32-34 However, serious side effects such as weight gain, fluid retention and fractures have limited the use of thiazolidinediones in clinical practice. Newer drugs such as glucagon-like peptide 1 agonists and dipeptidyl peptidase IV inhibitors hold promise in their ability to prevent diabetes,35,36 but they are expensive and have not been given to individuals with prediabetes for long periods of time. Pharmacological agents (mainly metformin) may be considered for younger people with prediabetes, in whom side effects are likely to be less troublesome and the potential advantage of delaying the onset of diabetes is likely to be greater. However, no drug currently has Therapeutic Goods Administration or Pharmaceutical Benefits Scheme approval for prediabetes within Australia.
Although prevention of diabetes is likely to have measurable health benefits for most people, this becomes less certain in the elderly. For example, the effect that diabetes has on reducing life expectancy diminishes with age, and is no longer apparent after the age of 80 years.37 Thus, intensive lifestyle intervention with the primary aim of preventing diabetes may not be appropriate for people with prediabetes in this age range. However, exercise programs with the primary aim of preserving physical and cognitive function and independence (i.e. not primarily focused on weight loss) are more likely to be of overall benefit in this older age group, and may still delay diabetes onset.
Barriers for diabetes prevention
Using data from the 2012 National Ambulatory Medical Care Survey, it was revealed that treatment (lifestyle modification counselling and/or use of metformin) was only indicated in the medical records in 23% of people with diagnosed or undiagnosed prediabetes.38 Understanding why treatment plans are infrequently provided to people with prediabetes is crucial for successful interventions to improve diabetes prevention. Data from a US sample of family physicians showed that physicians who have a positive
attitude toward prediabetes as a clinical construct are more likely to follow national guidelines for screening and recommend metformin to their patients with prediabetes. Most physicians also believed that a patient’s ability to modify lifestyle, economic resources, time for patient education on lifestyle modification and difficulty with sustaining patient motivation are significant barriers to prediabetes care.39 To improve diabetes prevention, a multifaceted approach that targets physicians’ understanding and compliance with guidelines as well as interventions to diminish patient barriers to diabetes prevention is necessary.
Conclusion
Prediabetes is a high-risk state for developing diabetes. Early detection and treatment of prediabetes is a fundamental strategy to prevent people from transitioning to diabetes. The two-stepped approach that is based on diabetes risk scores for the general population and further blood tests for those who are identified as having high-risk status can be recommended for prediabetes screening. If prediabetes is identified, a lifestyle intervention program should commence to prevent or slow the transition to diabetes. ET
Professor Shaw has received honoraria for lectures and consultancies from Astra Zeneca, Mylan, Merck Sharp and Dohme, Novo Nordisk, Eli Lilly, Boehringer Ingelheim and Sanofi.
References
30: e79; author reply e80.
1319-1328.
3230-3236.
with standing or walking attenuates the postprandial metabolic response in postmenopausal women: a randomized acute study. Diabetes Care 2016;
39: 130-138.
J Am Board Fam Med 2016; 29: 663-671.