Type 2 diabetes in pregnancy: what are the risks?

Diabetes type 2
Diabetes and pregnancy
Type 2 diabetes in pregnancy is common and associated with increased rates of serious adverse pregnancy outcomes. Increased awareness that this is a serious condition of pregnancy is of paramount importance. Preconception care and a multidisciplinary team approach throughout pregnancy are key to improving outcomes.
- Type 2 diabetes in pregnancy is an increasingly common condition, often undiagnosed prior to pregnancy.
- It is associated with increased rates of serious adverse pregnancy outcomes, including congenital anomalies and perinatal death.
- Women considering pregnancy and with risk factors for type 2 diabetes should be screened for diabetes prepregnancy and, if negative, be screened again in the first trimester.
- Preconceptive care with optimisation of metabolic control, assessment and management of diabetes complications, changing of medications to those safe for use in pregnancy and folic acid supplementation will have the greatest impact on improving outcomes.
- A multidisciplinary team approach is required, with clinicians experienced in managing diabetes in pregnancy, for optimal results for both mother and baby.
Picture credit: © Suriyapong Thongsawang/iStockphoto.com Model used for illustrative purposes only
The increasing prevalence of type 2 diabetes at younger ages translates into more pregnant women being affected, many of whom are undiagnosed prepregnancy. A review in 2005 indicated that the outcomes of pregnancies complicated by type 2 diabetes were similar or even worse than those complicated by type 1 diabetes, including increased rates of congenital anomalies and perinatal death.1,2 A recent Australian study concluded that type 2 diabetes in pregnancy was associated with significantly adverse obstetric and neonatal outcomes compared with pregnancies in women without diabetes, but there was no increased risk of congenital anomalies or perinatal death.3 This may be indicative of some improvement in the care of women with this condition; however, there is a long way to go to normalise outcomes.
This article discusses ways to improve outcomes in pregnant women with type 2 diabetes by increasing awareness that this is a serious condition, improving diagnosis of type 2 diabetes in high-risk women before conception, prepregnancy care and a multidisciplinary team approach during the pregnancy.
What are the risks of type 2 diabetes in pregnancy?
Congenital anomalies and perinatal deaths
An international review of the literature in 2005 concluded that type 2 diabetes in pregnancy is associated with significant increases in congenital anomalies and perinatal deaths.1 Among these was a study involving 180 pregnancies in women in Australia with type 1 or type 2 diabetes (55% of women had type 2 diabetes).2 There were six perinatal deaths, equating to 3.4% of the diabetes pregnancies, compared with a perinatal mortality rate of 0.7% in the background population. Importantly, five of the six perinatal deaths occurred in women with type 2 rather than type 1 diabetes. The rate of congenital anomalies within this same cohort was 10% for women with type 2 diabetes compared with 6% in women with type 1 diabetes and 2.1% in the background population.1,2
Interestingly, a more recent Australian study of 138 pregnancies in women with type 2 diabetes resulting in singleton births of more than 20 weeks’ gestation did not indicate a statistically significant increase in congenital anomalies or perinatal deaths compared with the background population.3 This could cautiously and optimistically be interpreted as an improvement achieved by increased awareness of the risks of type 2 diabetes and better management of such pregnancies. However, an alternative explanation could be a higher termination rate at less than 20 weeks’ gestation in women with type 2 diabetes as a consequence of earlier detection of congenital anomalies.
Other neonatal and maternal morbidities
The recent Australian study compared outcomes of 138 pregnancies in women with type 2 diabetes with 27,075 pregnancies in women without diabetes from 2010 to 2013.3 It showed increased rates of preterm birth (adjusted odds ratio [OR], 2.7; 95% confidence interval [CI], 1.8–4.2), large for gestational age (OR, 2.1; CI, 1.4–3.3), neonatal hypoglycaemia (OR, 4.9; CI, 2.8–8.6), jaundice (OR, 2.6; CI, 1.6–4.1) and shoulder dystocia (OR, 2.7; CI, 1.1–6.8).3 Women with type 2 diabetes also had higher rates of induction of labour (OR, 4.0; CI, 2.7–6.0), caesarean section (OR, 2.1; CI, 1.4–3.0) and pre-eclampsia (OR, 2.8; CI, 1.5–5.1).3
Similar findings were reported from a cohort of 274 pregnancies in women with type 2 diabetes audited between 2006 and 2009 in the UK.4 The adverse outcomes were similar to those that occur in women with type 1 diabetes, but the rates were lower in women with type 2 diabetes for large for gestational age (53% for type 1 diabetes vs 38% for type 2 diabetes; p<0.001) and premature delivery (37% for type 1 diabetes vs 18% for type 2 diabetes; p<0.0001).4
Characteristics of women with type 2 diabetes in pregnancy
The characteristics of women with type 2 diabetes in pregnancy reflect those of women with type 2 diabetes in the nonpregnant population.5 Affected women tend to be older, are overweight or obese and are likely to have a positive family history. Type 2 diabetes in pregnancy is also more likely to occur in women from ethnic groups with a higher background risk of type 2 diabetes, including Indigenous Australians, Pacific Islanders, South Asians, black Africans and those from the Middle East.
Other at-risk groups include women with a previous diagnosis of gestational diabetes, polycystic ovarian syndrome, mental health disorders and those who require assisted fertility treatment. Type 2 diabetes is very often accompanied by obesity, dyslipidaemia, pre-existing hypertension and at times obstructive sleep apnoea, all of which can impact on pregnancy outcomes.5 Furthermore, some of these women will have established microvascular and macrovascular complications.
Improving outcomes for women with type 2 diabetes
The value of prepregnancy care
There is ample evidence in women with type 1 diabetes that poor glycaemic control at the time of conception and through the first trimester is causative of congenital anomalies and predicts poorer outcomes. There is no reason to believe that this is any different for women with type 2 diabetes.5 It is therefore important that women at increased risk of type 2 diabetes present for a prepregnancy health check and that screening for diabetes be performed. This should include prepregnancy screening for diabetes in overweight and obese women being referred for assisted fertility treatments.
Clearly, all women known to have type 2 diabetes (or prediabetes) in the childbearing years should be advised to plan their pregnancies and have their condition optimised before conception. This should also include advice on contraception to avoid unplanned pregnancies.5 As well as optimisation of glycaemic control (target HbA1c ≤6.0% or ≤42 mmol/mol) through lifestyle measures and use of medications known to be safe in pregnancy, other medications should be reviewed and optimised for pregnancy and other comorbidities including the presence of diabetes complications should be assessed and stabilised. Diabetic retinopathy can progress rapidly during pregnancy and must be stabilised before pregnancy if present. Ischaemic heart disease is uncommon in women during pregnancy, but the consequences of undiagnosed ischaemic heart disease in pregnancy can be fatal such that this risk should be considered in the highest-risk women.
Folic acid should be started prepregnancy to reduce the risk of neural tube defects. The Australasian Diabetes in Pregnancy Society guidelines for management of pre-existing diabetes in pregnancy suggest a folic acid dose of 5 mg daily, which is very high.6 It is the practice of the author to recommend 1 mg daily prepregnancy and through the first trimester. This is due to a potential risk that higher doses could cause harm, particularly in women with low vitamin B12 status.7
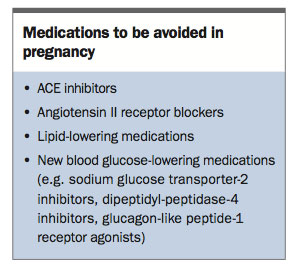
Medications that should be avoided in pregnancy are listed in the Box. Safe first-line antihypertensive agents for use in pregnancy include α-methyldopa and labetolol.8 Nifedipine slow release is commonly used as a second-line agent.8 Safe blood glucose-lowering agents are discussed below.
{kind=link}
Screening for undiagnosed diabetes early in pregnancy for at-risk women
Unfortunately, many women with risk factors for undiagnosed type 2 diabetes will present only once they are pregnant. Rather than waiting to 24 to 26 weeks’ gestation to screen for gestational diabetes, this group should have early pregnancy screening for diabetes as recommended by the World Health Organization.9 The optimal screening test for diabetes early in pregnancy is still being determined, but there is evidence from a New Zealand study that an HbA1c level of 5.9% or above (≥41 mmol/mol) is associated with adverse pregnancy outcomes and should be treated as gestational diabetes.10 An HbA1c level of 6.5% or above (≥48 mmol/mol) in early pregnancy should be considered diagnostic of overt diabetes in pregnancy. If the early screen is negative, an oral glucose tolerance test (OGTT) should be performed between 24 and 26 weeks’ gestation. The HbA1c test should not be used as a substitute gestational diabetes screening test for the OGTT at 24 to 26 weeks’ gestation.
Management of blood glucose in type 2 diabetes in pregnancy
Metformin and sulfonylureas should not be immediately ceased on confirmation of pregnancy. The rationale for this is that poor glycaemic control in the first trimester has clearly been associated with increased rates of congenital anomalies and miscarriages, whereas use of metformin and sulfonylureas have not.6 In most circumstances, insulin therapy will be required to optimise glycaemic control before weaning the oral hypoglycaemic agents, although metformin is continued throughout type 2 diabetes pregnancies in many centres. There is limited evidence on the safety of metformin in women with type 2 diabetes during pregnancy; however, the outcomes with metformin in gestational diabetes are reassuring.11 We await the results of the Metformin in Women with Type 2 Diabetes in Pregnancy Trial (MiTy).12
Lifestyle measures of healthy diet (particularly with avoidance of junk foods) and exercise, with assistance of a dietitian, are also keys to optimal outcomes in women with type 2 diabetes in pregnancy. Self-monitoring of blood glucose levels (BGL) is also essential to monitor progress and for therapy titration. The target for glycaemic control is as close to normal as is possible without causing unacceptable hypoglycaemia (e.g. fasting BGLs of ≤5.2 mmol/L, and two-hour postmeal BGLs of ≤6.7 mmol/L). Most women should be able to achieve HbA1c levels of less than 6.0% (<42 mmol/mol).
Prevention of excess maternal gestational weight gain
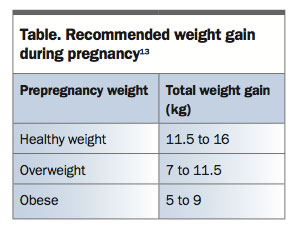
Evidence is mounting to suggest that gestational weight gain is an important factor, independent of glycaemia, in determining pregnancy outcomes in women with type 2 diabetes.13 Weight gain should be monitored with the aim to keep it well within the limits advised by the Institute of Medicine (Table).13
{kind=link}
Use of low-dose aspirin to prevent pre-eclampsia
Systematic reviews and meta-analyses support a benefit for use of low-dose aspirin therapy to reduce the complication of pre-eclampsia in high-risk pregnancies, including those complicated by pre-existing diabetes.14-16 Although the optimal timing and dose is still being determined, current evidence supports starting before 16 weeks’ gestation (after pregnancy viability has been confirmed by first trimester ultrasound) at a dose of 100 to 150 mg daily.
Maternal and fetal monitoring during pregnancy
In addition to blood glucose and weight monitoring, maternal blood pressure should be measured regularly. Vigilance for symptoms and signs of pre-eclampsia is important, as this condition is more common in women with type 2 diabetes. A first trimester nuchal translucency and blood test should be offered. Ultrasound should be performed for fetal morphology at 18 to 20 weeks, and for fetal growth at about 28 to 30 and 34 to 36 weeks’ gestation.6
Peripartum management
Induction of labour or need for caesarean section should be based on obstetric and/or fetal indications. If delivery is likely to be before 36 weeks, glycaemic control has not been adequate or obstetric concerns for delivery of a macrosomic infant are present, anticipate that neonatal intensive care unit facilities may be required. Insulin requirements fall rapidly during labour and in the puerperium. At this time, close monitoring and adjustment of insulin therapy is necessary. In many women with type 2 diabetes, insulin can be ceased immediately postpartum.
Antenatal care from a multidisciplinary team
Optimal care of women with type 2 diabetes in pregnancy requires a multidisciplinary team approach working closely with the general practitioner. The team in major centres will usually comprise diabetes management clinicians (dietitian, diabetes nurse educator and endocrinologist), the obstetric team (midwife, obstetrician, fetal medicine physician and anaesthetist) and the neonatology team. Access to other specialties including ophthalmology, sleep medicine and cardiology should also be available. It is important that solutions are put in place for women from rural and remote regions to provide equal quality care through upskilled general practitioners and general physicians, and partnering with larger centres, such as through the use of telehealth. Timely transfer of care should be undertaken to major centres for higher-risk pregnancies.
Conclusion
Although there may be some indications that pregnancy outcomes for women with type 2 diabetes are improving, normalisation of outcomes is a long way off. Increasing the awareness that type 2 diabetes in pregnancy is a serious condition is the first step. Improved diagnosis of type 2 diabetes in high-risk women before conception, as well as pregnancy planning and care by expert multidisciplinary teams, are likely to have the most impact on improving outcomes.
Acknowledgement
The author would like to thank Dr Jacqueline Jones, Junior Medical Officer at The Canberra Hospital, Canberra, ACT for her useful comments and proof reading of this article.
References
- Cheung NW, McElduff A, Ross GP. Type 2 diabetes in pregnancy: a wolf in sheep’s clothing. Aust N Z J Obstet Gynaecol 2005; 45: 479-483.
- McElduff A, Ross GP, Lagstrom JA, et al. Pregestational diabetes and pregnancy: an Australian experience. Diabetes Care 2005; 28: 1260-1261.
- Abell SK, Boyle JA, de Courten B, et al. Impact of type 2 diabetes, obesity and glycaemic control on pregnancy outcomes. Aust N Z J Obstet Gynaecol 2017; 57: 308-314.
- Murphy HR, Steel SA, Roland JM, et al. Obstetric and perinatal outcomes in pregnancies complicated by type 1 and type 2 diabetes: influences of glycaemic control, obesity and social disadvantage. Diabet Med 2011; 28: 1060-1067.
- Temple R, Murphy H. Type 2 diabetes in pregnancy - an increasing problem. Best Pract Res Clin Endocrinol Metab 2010; 24: 591-603.
- McElduff A, Cheung NW, McIntyre HD, et al. The Australasian Diabetes in Pregnancy Society consensus guidelines for the management of type 1 and type 2 diabetes in relation to pregnancy. Med J Aust 2005; 183: 373-377.
- Boyles AL, Yetley EA, Thayer KA, et al. Safe use of high intakes of folic acid: research challenges and paths forward. Nutr Rev 2016; 74: 469-474.
- Lowe SA, Bowyer L, Lust K, et al. SOMANZ guidelines for the management of hypertensive disorders of pregnancy 2014. Aust N Z J Obstet Gynaecol 2015; 55: e1-e29.
- Agarwal MM, Boulvain M, Coetzee E, et al. Diagnostic criteria and classification of hyperglycaemia first detected in pregnancy: a World Health Organization Guideline. Diabetes Res Clin Pract 2014; 103: 341-363.
- Hughes RC, Moore MP, Gullam JE, et al. An early pregnancy HbA1c ≥5.9% (41 mmol/mol) is optimal for detecting diabetes and identifies women at increased risk of adverse pregnancy outcomes. Diabetes Care 2014; 37:
- 2953-2959.
- Rowan JA, Hague WM, Gao W, et al. Metformin versus insulin for the treatment of gestational diabetes. N Engl J Med 2008; 358: 2003-2015.
- Feig DS, Murphy K, Asztalos E, et al. Metformin in women with type 2 diabetes in pregnancy (MiTy): a multi-center randomized controlled trial. BMC Pregnancy and Childbirth 2016; 16: 173.
- Blackwell SC, Landon MB, Mele L, et al. Relationship between excessive gestational weight gain and neonatal adiposity in women with mild gestational diabetes mellitus. Obstet and Gynecol 2016; 128: 1325-1332.
- Duley L, Henderson-Smart DJ, Meher S, et al. Antiplatelet agents for preventing pre-eclampsia and its complications. Cochrane Database Syst Rev 2007; (2): CD004659.
- Meher S, Duley L, Hunter K, et al. Antiplatelet therapy before or after 16 weeks’ gestation for preventing preeclampsia: an individual participant data meta-analysis. Am J Obstet Gynecol 2017; 216: 121-128. e2.
- Roberge S, Nicolaides K, Demers S, et al. The role of aspirin dose on the prevention of preeclampsia and fetal growth restriction: systematic review and meta-analysis. Am J Obstet Gynecol 2017; 216: 110-120. e6.