The GP's role in postfragility fracture management

Fractures
Osteoporosis
Osteoporosis is characterised by low bone mineral density and architectural deterioration which leads to reduced bone strength and increased fracture risk. This progressive process has no symptoms and is therefore frequently underdiagnosed, often first presenting with a minimal trauma fracture.
- Despite the availability of safe and effective treatments there is a large evidence-practice gap in osteoporosis care, including following minimal trauma fracture.
- All men from 50 years of age and all postmenopausal women (without a minimal trauma fracture) should be screened for risk factors for osteoporosis; some will warrant bone mineral density testing.
- All patients who experience a fracture from minimal trauma should be assessed for osteoporosis.
- Patients taking oestrogen or androgen deprivation therapy or those taking steroids for more than three months are at high risk of osteoporosis.
- Always consider secondary causes of osteoporosis in patients affected by low bone mineral density and systematically exclude potential contributors.
- Ongoing monitoring should focus on diet, safe sun exposure, exercise and harmful medications; falls risk reduction and osteoporosis medication adherence should be reviewed.
Osteoporosis underlies many preventable fractures. Yet it has multiple safe and effective treatments that are readily available and supported by strong evidence for fracture prevention and some evidence for reduction in mortality.1,2 Despite this, osteoporosis remains underrecognised and undertreated. Comprehensive information on work-up, diagnosis and specific medications is readily available and therefore not covered in this article. Instead, we will focus on several important issues for the GP to be aware of using two case scenario discussions as examples.
Reduced bone strength in patients often first presents with a minimal trauma fracture. Yet even after a minimal fracture, it is estimated that 70 to 85% of patients are neither assessed nor treated for osteoporosis.3
Both morbidity and mortality are increased after all minimal trauma fractures, with hip fractures having the greatest impact.4,5 In addition, it is estimated that subsequent fracture risk is two to four times higher after an initial minimal trauma fracture.6 Subsequent fracture risk is significantly reduced (more than 40% relative risk reduction) with targeted osteoporosis treatments, yet less than 30% of women and 10% of men diagnosed with osteoporosis are receiving appropriate treatment.1,7 There is some (but limited) evidence of a mortality benefit in a small number of studies.2
The number-needed-to-treat is lower in those with a high absolute risk of fracture. It follows that a focus on ensuring that any person with a fragility fracture is appropriately managed is a high value activity for primary and secondary care clinicians. A practice audit for people more than 50 years of age who have had a fracture will likely yield many undertreated cases.
Case scenario 1: a case of secondary prevention
Liz, 70 years, presents after recently being discharged from the local hospital. Four weeks earlier she had slipped on a rug while at home and fallen onto her right knee, sustaining a minimally displaced fracture of the distal right femur. She was admitted to hospital and placed in a range-of-motion knee brace, with gradual mobilisation. She was then transferred to the rehabilitation unit for two weeks of physiotherapy, occupational therapy and discharge planning. What needs to be addressed in this follow-up consultation?
Identifying patients at risk
One of the most important aspects of improving osteoporosis management is increasing identification of patients at high risk and ensuring appropriate evaluation and investigation. Patients with the highest risk of underlying osteoporosis are those presenting with a minimal trauma fracture, therefore all men from 50 years of age and postmenopausal women who sustain a minimal trauma fracture should be presumed to have a diagnosis of osteoporosis and undergo assessment for underlying risk factors and investigation (secondary fracture prevention).1 To identify other patients potentially at risk (including primary fracture prevention), the 2017 RACGP Clinical guideline for the prevention and treatment of osteoporosis in postmenopausal women and older men recommends all men from 50 years of age and postmenopausal women should be screened for risk factors for osteoporotic fracture (see Box 1).1
{kind=link}
An important (and growing) group for GPs to consider is patients on oestrogen or androgen deprivation therapy, usually for breast or prostate cancer. Women and men taking hormone blockade have accelerated bone loss with premenopausal women experiencing the greatest increase in the rate of bone loss.8 All patients should have a baseline bone mineral density (BMD) assessment before commencing hormone blockade. Patients on oral glucocorticoids have a similarly high risk and warrant similar attention.
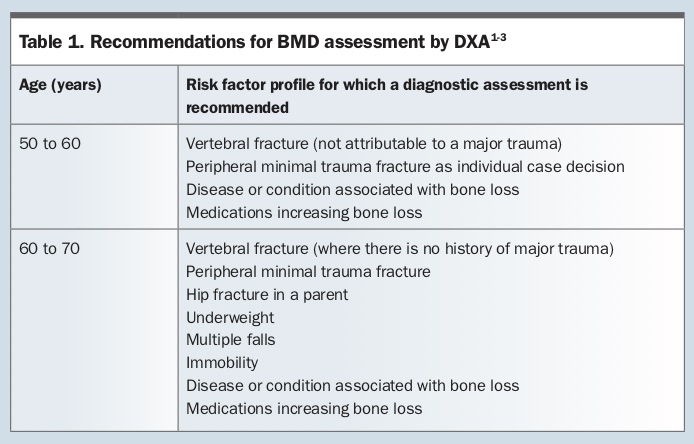
Complete diagnostic evaluation should include medical history, clinical assessment, BMD by dual energy x-ray absorptiometry (DXA) and appropriate blood tests and radiographs as indicated. Table 1 outlines recommendations for BMD based on these risk factor assessments.
{kind=link}
Case scenario 1 continued
Important aspects to follow up in the consultation are:
- identifying that Liz most likely has underlying osteoporosis and screening for other risk factors and investigating BMD
- further falls prevention including ensuring an occupational therapy home assessment has been completed and referral to a falls prevention program
- ongoing management at home, need for temporary postacute care package and possible referral to an aged care assessment team
- support her confidence to become active again because exercise should be a key component of falls prevention and fracture risk reduction.
Liz could not remember having a scan for her BMD during admission, and there was no mention of this in the discharge summary. During the initial consultation, Liz’s medical file was also reviewed: there is no significant past medical history, she is not taking any regular medications and she has had two previous falls in the past 12 months but no previous fractures. She is a smoker of about 10 cigarettes per day and drinks one to two standard drinks per week. She has a diet rich in calcium. She does not do much regular, structured exercise. She manages completely independently living at home by herself.
Liz refused referral to an aged care assessment team or a falls prevention program, but an occupational therapy home assessment and adjustments were made while she was in rehabilitation.
Physical examination with attention to gait, balance and vision was unremarkable.
Liz initially declined to go ahead with a DXA scan for assessing her BMD, but after discussing the increased risk of underlying osteoporosis and further fracture after this initial event she agreed to have this done.
Liz’s DXA results revealed a lumbar spine T-score of –2.0 and hip T-score of –2.1. She is osteopenic and with a minimal trauma fracture fulfils the PBS criteria for a diagnosis of ‘established osteoporosis’ and also fulfils criteria for treatment with an osteoporosis- specific therapy.
Pharmacological treatment
There are many recommended first-line pharmacological treatments for osteoporosis and no head-to-head trials to demonstrate superiority of one over another. Greatest adherence will generally be achieved through a process of open discussion of different appropriate treatment options and shared decision-making. In case scenario 1 – after discussion over two visits – Liz’s preference was to commence denosumab six-monthly injections. Bisphosphonates would have been an equally appropriate treatment choice. Due to her age (and years postmenopause), oestrogen replacement therapy would not be ideal due to a higher risk-benefit profile with more than 10 years postmenopause.
RACGP recommendations for the treatment of postmenopausal women are available at www.racgp.org.au/download/Documents/Guidelines/Musculoskeletal/osteoporosis-algorithm.pdf.
Case scenario 2: a case of primary prevention
Sue, 70 years, presents with the exact same history as Liz in case scenario 1, but no fracture during her last fall, that is:
- she has had two previous falls this year, but no previous fractures
- there is no significant past medical history
- she is not taking any regular medications
- she is a smoker – about 10 cigarettes per day
- she drinks one to two standard drinks per week
- her diet is rich in calcium
- she does not take much regular, structured exercise
- she manages completely independently living at home by herself.
Sue’s BMD scores revealed a lumbar spine T-score of –2.0 and hip T-score of –2.1. How should Sue be advised?
Making treatment choices
Treatment with osteoporosis-specific pharmacotherapy is recommended with T-scores less than –2.5 on DXA, a minimal trauma fracture of the vertebra or hip regardless of BMD, or osteopenia on BMD with a minimal trauma fracture at any other site.1 The decision to recommend treatment is often easy with patients who meet the above criteria. However, the decision can be more difficult in those with intermediate risk or borderline BMD. The interpretation of risk is personal, and the thresholds for recommending treatment are thinly based on evidence of likely cost effectiveness.
In this situation, a patient’s absolute fracture risk can be estimated to assist in the treatment decision. It is important to note that absolute fracture risk gives an idea of the percentage risk of fracture over a specified period of time. This is in contrast to relative risk, which calculates a person’s risk of fracture compared with a reference group. Absolute risk calculation gives a more accurate indication of individual risk and it is simple to describe what a 40% reduction in that risk would be if on appropriate pharmacotherapy.
Both the Fracture Risk Assessment Tool (FRAX) and the Garvan Fracture Risk Calculator (GFRC) are readily available and commonly used.9,10 Box 2 outlines their components. Note that neither takes into account patients on oestrogen or androgen deprivation therapy and therefore the risk in this group may be underestimated. A discussion of their specifics and limitations is beyond the scope of this article; however, clinicians should use the calculator that they feel most suits the clinical particular situation.11 Benefit of their use has not been proven in prospective trials, but they have predictive value good enough to aid patient education and choice.11 While high fracture risk does not currently directly enable PBS prescription, it can facilitate treatment decisions. For example, an osteopenic patient without a history of fracture but with a high absolute fracture risk is likely to benefit from treatment and commencing specific pharmacotherapy should be considered. Calculating absolute fracture risk with patients is also a powerful tool for shared decision- making, and therefore increased patient adherence and ownership of management.
{kind=link}
Case scenario 2 continued
On hearing that she did not have osteoporosis, Sue declined treatment. However, her fracture risk was calculated using the GFRC. This revealed a 12% 10-year risk of hip fracture and a 31% 10-year risk of any fragility fracture. At this level of risk, for this calculator (3 to 9% 10-year hip fracture risk and 14 to 26% 10-year risk of any osteoporotic fracture), treatment is likely to be beneficial and is recommended. This risk was discussed with Sue and the recommendation to treat at this level of risk explained. Sue was shown how her relative risk of hip fracture could be reduced by about 40% with some treatments (translating to an absolute risk reduction of 4.8%, thus a number-needed-to-treat of about 20).1 After this discussion, Sue decided to start treatment, even though it is not PBS subsidised.
A wholistic approach, other elements of treatment
Effective management of osteoporosis should address all aspects of bone heath and fracture risk, including:
- calcium and vitamin D: high calcium diet (preferable) and/or low-dose supplements (if unable to achieve 1000 mg daily in diet); vitamin D supplementation as appropriate
- smoking cessation and alcohol reduction
- weight-bearing exercise or resistance training
- falls prevention – physiotherapy or exercise physiologist for strength and balance training, occupational therapy and/or specific falls prevention programs
- consider ceasing or rationalising mediations which can reduce bone density or increase the risk of falls.
Long-term monitoring
Long-term follow up of patients with borderline BMD should identify any increased or new risk factors and monitor fracture risk. This should be an opportunity to re-enforce general measures to improve bone health and reduce falls risk. Repeating BMD should only be considered if the result is likely to change treatment decisions. At least two years is needed to see a change in BMD that is greater than the error inherent in BMD testing, and there is evidence for delaying repeat DXA until five years or more when baseline BMD is above the osteopenic range and in the absence of bone-losing medication (Box 1) or conditions associated with bone loss.1,12
For patients taking anti-osteoporosis medications, follow up should similarly review general bone health measures and fracture risk and review medication adherence and any issues around this, as well as any medication side effects. The ongoing need to continue anti-osteoporosis medication should be reviewed. Treatment should not be stopped if BMD T-score remains less than –2.5. Although repeat BMD assessment while on treatment is generally not useful or necessary, there may be situations where it can help with medication adherence. Changes in BMD while on treatment do not correlate usefully with changes in fracture risk.
Conclusion
GPs are uniquely placed to help close the evidence-practice gap in osteoporosis. Most hospital systems will soon be implementing programs to increase the identification and initiation of management of osteoporosis in cases that first present in this setting. However, most fragility fractures will not be admitted, or even present to hospital (particularly compression vertebral fractures), therefore GPs need to be systematic in identifying cases and confident in initiating and maintaining treatment. ET