Iodine-induced thyroid disease

Thyroid diseases
Endocrine diseases
The immediate management and investigation of an acute endocrine presentation in general practice is discussed in this section. It is inspired by, but not based on, a real patient situation.
What is your initial impression?
Answer: Amanda’s symptoms could be caused by several medical problems. Palpitations are a sensory symptom of an unpleasant awareness of the beating of the heart. It is helpful to get the patient to clarify the experience, including a description of heart rate, regularity, onset and duration. The cause of Amanda’s symptoms could be cardiac, metabolic (thyrotoxicosis, hypoglycaemia), psychiatric, medication or drug-related. Other potential causes are high-output states (e.g. anaemia) or states of catecholamine excess (e.g. exercise, stress, phaeochromocytoma).1 In Amanda’s case, the combination of palpitations, anxiety, weight loss, diarrhoea and recent iodine supplementation make hyperthyroidism an important condition to consider.
What other information do you need from the history?
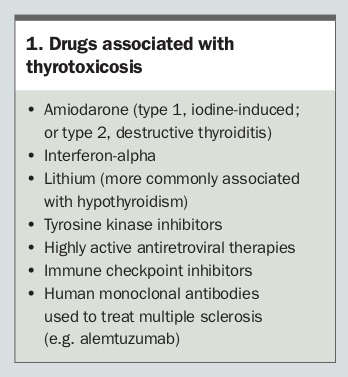
Answer: Red flags for a cardiac cause of the palpitations would need to be excluded, such as their association with syncope or a family history of sudden death. A thorough medication and drug history is essential to exclude other causes of Amanda’s symptoms (e.g. alcohol, caffeine, other stimulants or drugs associated with prolongation of the QT interval). Given her history of iodine supplementation, it would be helpful to search for a history of exposure to other iodine-containing agents including amiodarone, radiographic contrast agents, other supplements such as nori or kelp and other medications that can be associated with thyrotoxicosis (Box 1).
{kind=link}
What are the key features you will assess on physical examination?
Answer: Your general examination of Amanda during your consultation will give clues about whether she is acutely unwell, as will the assessment of her vital signs including blood pressure, heart rate and rhythm, respiratory status and temperature. Thorough cardiopulmonary and abdominal examinations should be conducted, and a search for peripheral signs of hyperthyroidism and examination of the thyroid gland are warranted.
Amanda is slim, with a weight of 51 kg and body mass index of 19.5 kg/m2. She appears comfortable and is not in any respiratory distress. Her peripheries are quite warm and she has a high-frequency tremor of the hands. Inspection of her face does not reveal any signs of exophthalmos or lid retraction. Her pulse is regular but fast at 96 beats per minute. Her blood pressure is 110/60 mmHg without a postural drop. Cardiac examination confirms regular tachycardia but no evidence of other structural or valvular abnormalities. Her chest auscultation reveals normal vesicular breath sounds throughout both lung fields. Abdominal examination is also unremarkable. There is evidence of some mild proximal weakness, with normal reflexes. On examination of her neck, there is a smooth, nontender thyroid gland without clinically detectable nodules, bruits or thrills and no cervical lymphadenopathy.
In summary, Amanda presents with symptoms suggestive of hyperthyroidism. She requires further evaluation for this condition.
How is hyperthyroidism defined and what are the possible causes?
Answer: Hyperthyroidism is considered overt or subclinical, depending on the results of biochemical testing. Overt hyperthyroidism is defined as a subnormal (usually undetectable) serum thyroid stimulating hormone (TSH) level with elevated serum levels of triiodothyronine (T3) and/or free thyroxine (free T4). Subclinical hyperthyroidism is defined as a low or undetectable serum TSH with T3 and free T4 values within their respective reference ranges. Primary hyperthyroidism can occur due to:
- excessive stimulation of the thyroid gland
- autonomous excess thyroid hormone synthesis and secretion
- passive release of preformed thyroid hormone in excess amounts
- exogenous thyroid hormone excess (Box 2).2,3
{kind=link}
The prevalence of overt hyperthyroidism is between 0.1 to 2.5% in iodine-sufficient countries.3
You explain to Amanda that you suspect the cause of her symptoms is hyperthyroidism.
What biochemistry tests are appropriate?
Answer: A full blood count and tests for thyroid function, liver function and thyroid autoantibodies and measurement of C-reactive protein, electrolytes, urea and creatinine levels are needed. Keep in mind that the prevalences in the normal population of thyroperoxidase and thyroglobulin antibodies are 11% and 5%, respectively.4 TSH receptor antibodies need to be specifically requested on the pathology form in cases of thyrotoxicosis as they are not routinely included in a request for thyroid autoantibodies.
Amanda’s thyroid function test results are as follow:
- TSH, <0.005 mIU/L (reference range [RR], 0.40-4.00 mIU/L)
- Free T4, 26.9 pmol/L (RR, 9.0-19.0 pmol/L)
- Free T3, 7.9 pmol/L (RR, 2.6-6.0 pmol/L)
These results are indicative of overt hyperthyroidism. Amanda’s thyroperoxidase antibody level was elevated at 20 kIU/L (RR, <5.6 kIU/L). A TSH receptor antibody test was negative.
What imaging would you consider?
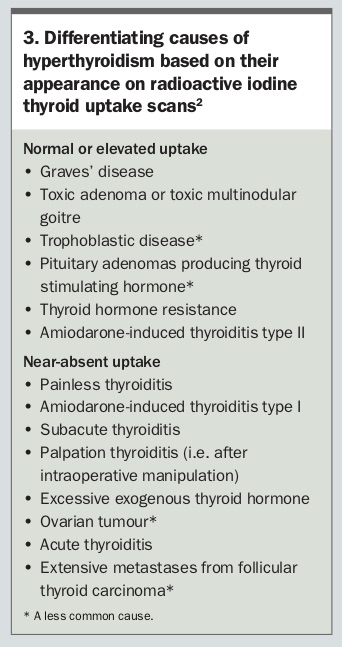
Answer: Radioactive iodine uptake scans can help distinguish the cause of hyperthyroidism (Box 3).2 They measure the percentage of administered radioisotope that is concentrated into the thyroid tissue. The uptake scan will help differentiate between causes that have elevated or normal uptake from those that have near-absent uptake.2 Uptake is diffusely elevated in Graves’ disease and normal or high (in some parts of the gland) in toxic multinodular goitre. The uptake will be near-absent in painless, postpartum or subacute thyroiditis, factitious hyperthyroidism and recent excess iodine intake. Furthermore, the uptake may be low after exposure to an iodinated contrast agent, amiodarone or ingestion of a diet unusually high in iodine in the preceding one to two months.
{kind=link}
In some patients, a thyroid ultrasound may be able to differentiate thyroid hyperactivity from destructive thyroiditis. This may be useful when a thyroid uptake scan is contraindicated, such as during pregnancy. If a thyroid uptake scan is needed in a woman who is breastfeeding her baby, breast milk can be expressed and stored ahead of time so milk expressed over the 12 hours after the radioisotope dose can be discarded.
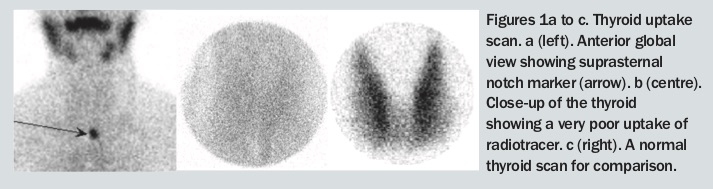
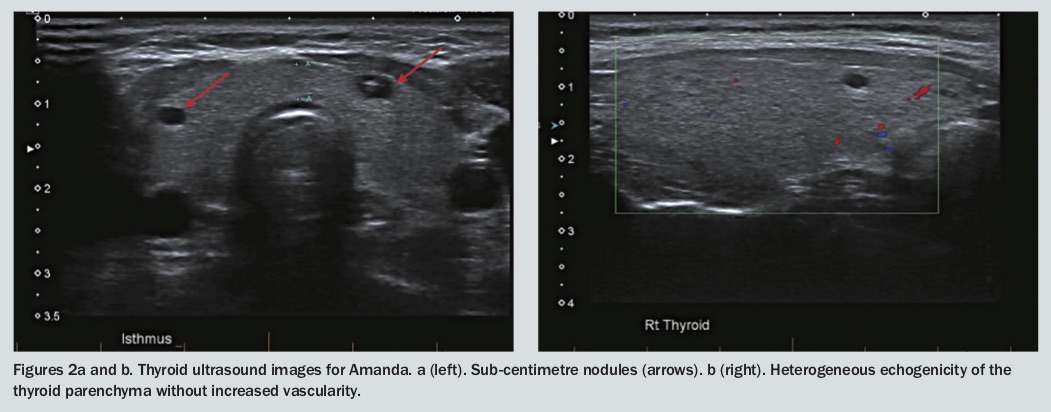
In Amanda’s case, her thyroid scan showed absent uptake, which is likely to be related to her recent prolonged excess ingestion of iodine supplements (Figure 1). A thyroid ultrasound is also performed. This shows a right lobe with a volume of 9.3 mL and left lobe measuring 5.3 mL. The overall vascularity of the gland is decreased and there are no suspicious cervical lymph nodes. Overall echogenicity is described as heterogeneous, consistent with thyroiditis (Figure 2). There are two small nodules. The one in the left lower lobe measures 4 x 5 x 3 mm, is predominantly spongiform and is categorised as having an ultrasound pattern fitting the American Thyroid Association very low suspicion category. The other is in the left mid lobe, measures 8 x 7 x 4 mm, is cystic and is reported as benign.
{kind=link}
{kind=link}
What do you think is the cause of Amanda’s hyperthyroidism? What is the relevance of the history of iodine supplementation?
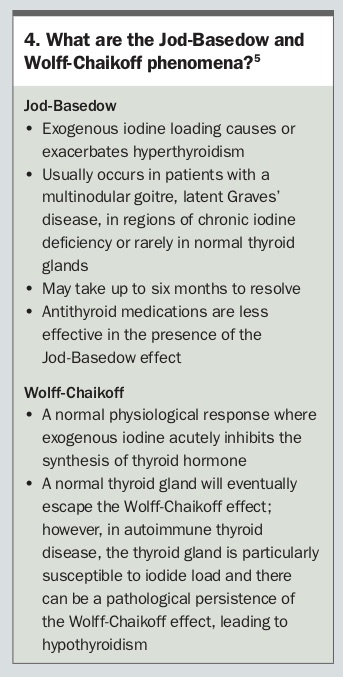
Answer: Amanda most likely has iodine-induced hyperthyroidism with a possible background of autoimmune thyroiditis. It is possible that the recent iodine supplementation unmasked a pre-existing state of subclinical or mild hyperthyroidism. This is known as the Jod-Basedow effect (Box 4).5
{kind=link}
In iodine-sufficient areas, iodine-induced thyroiditis usually occurs in the setting of a pre-existing multinodular goitre or latent Graves’ disease. The elderly may be particularly vulnerable. Rarely, it may occur in patients without underlying thyroid disease.
What is the relevance of the nodules seen on the ultrasound and do they require further follow up?
Answer: Amanda’s thyroid nodules are a potential predisposing risk factor for her current iodine-induced hyperthyroidism, but the nodules themselves do not require any further evaluation or any ongoing monitoring.
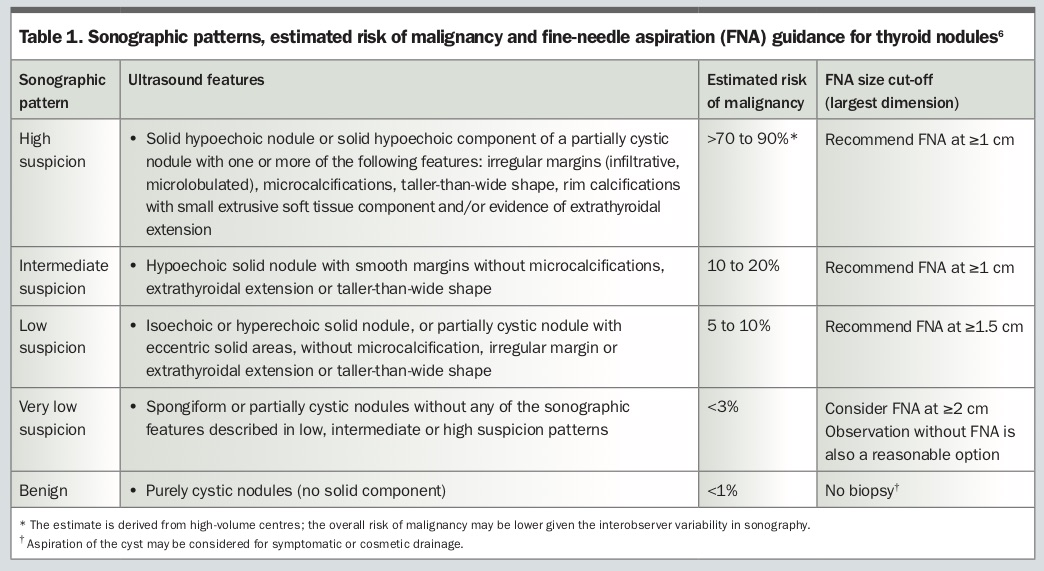
Most thyroid nodules are low risk. Generally, only nodules that measure more than 1cm with sonographic features of concern should be evaluated, as clinically significant thyroid cancer in smaller nodules is very rare.6 There are several sonography-based risk-stratification guidelines aimed at identifying thyroid nodules that require fine-needle aspiration for further evaluation. Two of these guidelines are the American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer (Table 1) and the American College of Radiology Thyroid Imaging Reporting and Data System.6,7
{kind=link}
What effects does iodine have on the thyroid gland?
Answer: Iodine is a key component of thyroid hormones. Iodine is available in food or water as iodide or iodate (iodate is then converted to iodide in the stomach). Iodide is actively transported from the circulation into thyroid follicular cells, where it can be stored and used for thyroid hormone synthesis. The WHO recommendations for daily intake are 150 mcg for adults, 250 mcg during pregnancy and lactation and 90 to 120 mcg for children, depending on age.8 Although iodide is an essential substrate for thyroid hormone synthesis, in an otherwise normal thyroid gland excess iodide paradoxically inhibits thyroid hormone production (the Wolff-Chaikoff effect) and thyroid hormone release from the gland.5 These inhibitory actions are transient and the normal thyroid gland escapes from these effects of excess iodide after 10 to 14 days. These autoregulatory effects of iodide protect thyroid function from short-term fluctuations in iodine intake.5
However, even modest increases in iodine supply can trigger hyperthyroidism in susceptible individuals. As mentioned previously, this may occur in the setting of nodular goitres (predominantly in elderly people after long exposure to iodine deficiency), after Graves’ disease and, less commonly, in normal thyroid glands. A high urinary excretion of iodine in a spot urine sample identifies iodine excess.9
How will you manage Amanda’s hyperthyroidism?
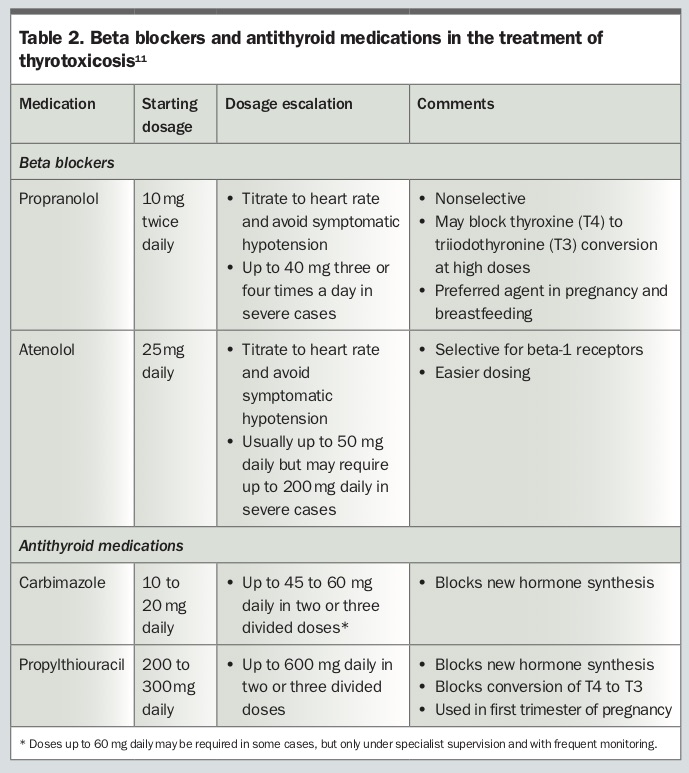
Answer: In the first instance, Amanda’s iodine supplementation should be ceased immediately and additional iodine exposure should be avoided. Given the features of tachycardia, palpitations, tremor and weight loss, Amanda’s condition warrants pharmacological management. Symptomatic thyrotoxicosis in iodine- induced hyperthyroidism should be managed with beta blockers and/or antithyroid medications.2 Antithyroid medications block thyroid hormone synthesis, and hence are useful when thyrotoxicosis is caused by excessive production and release of thyroid hormones, as in iodine-induced hyperthyroidism and in type 1 amiodarone-induced thyrotoxicosis.10 Beta blockers are relatively contraindicated in bronchospastic asthma, although a nonselective beta blocker could be used cautiously to treat thyrotoxicosis with strict monitoring of pulmonary status in judiciously selected patients. Suggested dosages of commonly used beta blockers and antithyroid medications are given in Table 2.11
{kind=link}
Carbimazole is the preferred antithyroid medication due to its long duration of action, once-daily dosing, more rapid efficacy and lower incidence of side effects; however, propylthiouracil should be used in the first trimester of pregnancy. Thyroid function tests should be reviewed at four to six weeks and then every three months. Serum TSH concentrations can remain suppressed for several months after hyperthyroidism is corrected, so initial dose adjustment should be based on the decrease in serum T3 and T4 concentrations rather than serum TSH level. As mentioned previously, antithyroid medications may be less effective in iodine-induced hyperthyroidism. Monitoring of urinary iodine levels adjusted for urine creatinine concentration can be considered for assessing the clearance of the iodine load.2 This is not essential, however, as over time the iodine levels would be expected to drop in the absence of continued iodine exposure.
Amanda is commenced on propranolol 10 mg twice daily. When reviewed by her endocrinologist six weeks later, she has continuing symptoms and weight loss. Her repeat thyroid function tests show little change and ongoing hyperthyroidism. Her propranolol dose is increased to 10 mg three times daily and she is commenced on carbimazole, initially at a total daily dose of 15 mg and subsequently increased up to 30 mg daily. She is advised to avoid strenuous physical activity until her cardiac symptoms stabilise. Her urinary iodine level settles within the mild-deficiency range and propranolol is gradually weaned when her cardiac symptoms subside. At this time she has regained 10 kg in weight.
You review Amanda six weeks later and she is feeling lethargic and generally unwell. You order repeat thyroid function tests.
What treatment will you initiate in response to the repeat test results?
Answer: A repeat set of Amanda’s thyroid function tests shows a TSH level of 9.00 mIU/L (RR, 0.40-4.00 mIU/L), a free T4 level of 8.0 pmol/L (RR, 9.0-19.0 pmol/L) and a free T3 level of 3.3 pmol/L (RR, 2.6-6.0 pmol/L). It is common to see resistance to antithyroid medications in the case of iodine-induced hyperthyroidism. As the iodine load dissipates, the sensitivity to these medications will increase. To manage this, her carbimazole dose needs to be gradually weaned, with regular clinical assessment and monitoring of her thyroid function tests every three months.10 ET