Menopause: how does it affect diabetes?

Menopause
Available evidence from randomised controlled trials suggests that menopausal hormone therapy (MHT) in postmenopausal women improves glucose homeostasis and reduces the risk of type 2 diabetes. Although the primary indication for MHT is alleviation of menopausal symptoms, clinical trial evidence can help inform the risk–benefit considerations around prescribing MHT.
- Menopausal hormone therapy (MHT) is principally indicated for the alleviation of troublesome menopausal symptoms. It should not be used as a treatment for diabetes, although clinical evidence can help inform the risk–benefit considerations around prescribing MHT.
- Evidence suggests that oestrogen-only MHT may reduce the incidence of coronary heart disease and type 2 diabetes in postmenopausal women without diabetes who have undergone a hysterectomy and are aged 50 to 59 years or within 10 years of their last period. For women in this group who have an intact uterus, MHT combining oestrogen with a progestogen has a neutral to beneficial effect on both coronary heart disease and on the incidence of type 2 diabetes.
- For women with diabetes aged 50 to 59 years or within 10 years of their last period, evidence suggests that oral oestrogens are more effective than transdermal oestrogens at improving glucose homeostasis and lipid profiles.
- The International Menopausal Society recommends that the mode of delivery of MHT is based on individual patient risk factors and preferences. However, oral oestrogens are a first choice only in women with a low risk of cardiovascular disease. Transdermal oestrogen delivery is preferred in women with or without type 2 diabetes who have an increased risk of cardiovascular disease or who are obese.
- A neutral progestogen should be a first choice in combined MHT to maximise the beneficial effects of oestrogen on glucose homeostasis and lipid profiles.
- MHT should only be initiated after careful consideration of all risk factors in postmenopausal women who are older than 60 years or more than 10 years from their last period.
*Refer to the text and relevant references provided for levels of clinical evidence for the recommendations.
Picture credit: © Fertnig/iStockphoto.com Model used for illustrative purposes only
The incidence of type 2 diabetes has reached epidemic proportions worldwide. It has been estimated that up to 50% of the US population are now either diabetic or have insulin resistance.1 In Australia, it is estimated that 1 million people – 4.4% of the population – have type 2 diabetes.2 In addition, most populations in western societies are ageing, which is likely to further increase the incidence of both type 2 diabetes and the population of women who are menopausal.
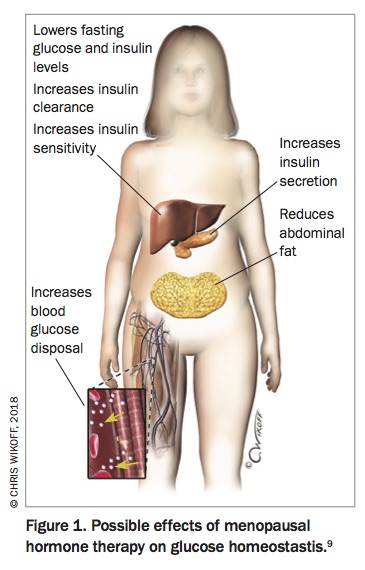
Large randomised controlled trials (RCTs) have suggested that menopausal hormone therapy (MHT) reduces the incidence of type 2 diabetes in women.3-7 The mechanisms by which this effect is mediated remain uncertain (Figure 1) and so the clinical implications of this effect are still controversial.8,9 Both RCTs and observational studies have largely studied women passing through a natural menopause transition. In contrast, most bench-top studies using rodents utilise a surgical model to investigate the mode of action of oestrogen in reducing the onset of type 2 diabetes. These models may induce different effects to the changes seen with a natural, slowly progressive, nonsurgical menopause.9
{kind=link}
Effects of menopause on type 2 diabetes
Fat distribution
Weight gain is a major health concern for women at midlife. Cross-sectional and longitudinal studies show that menopause is associated with a preferential increase in intra-abdominal fat that is independent of age and total body fat mass. This is thought to be due to a decreased metabolic rate without any change in food intake. Energy expenditure also decreases with age and this decrease is greater in postmenopausal women than in premenopausal controls.10
The menopause therefore is marked by a decrease in energy expenditure and an increase in total body and abdominal fat without changes in energy intake. A likely mechanism for this is decreased estradiol levels as a result of menopause, which leads to a reduced activation of oestrogen receptor alpha in the hypothalamus. This, in turn, impairs the ability of the sympathetic nervous system to regulate fat distribution.11
Obesity is an independent risk factor for metabolic disease and also for worsening menopausal symptoms. The most effective treatment for these symptoms is MHT, which also does not increase abdominal fat. Metformin is a useful drug for selected overweight individuals who have diabetes or are at risk of diabetes. Successful management of weight loss always involves appropriate lifestyle changes.12
Glucose homeostasis
The relationship between menopause and diabetes risk remains controversial. The Study of Women’s Health Across a Nation (SWAN study) argued that the adverse changes in blood glucose and insulin levels seen in women in midlife were more about chronological than ovarian ageing.13 However, long-term observational studies of French and Chinese women experiencing premature menopause before the age of 40 years showed that these women were 20% (odds ratio [OR], 1.20; 95% confidence interval [CI], 1.03–1.39) to 32% (hazard ratio [HR], 1.32; 95% CI, 1.04–1.69) more likely to develop diabetes than women whose menopause occurred at the normal age of around 51 years.9 Longitudinal studies in women undergoing surgical menopause also point to an approximate 50% increased risk of developing diabetes compared with women who experienced a natural menopause, irrespective of age.
Recently an examination of 124,379 postmenopausal women participating in the Women’s Health Initiative demonstrated that cumulative life exposure to oestrogen was a determinant of diabetes risk.14 After adjustment for age, women with the lowest lifetime exposure to oestrogen (<30 years) had a 37% greater risk of developing type 2 diabetes than women whose lifetime exposure was 36 to 40 years. Interestingly, women with the longest period of exposure to reproductive hormones and thus a later onset of menopause also had an increased risk of diabetes – 23% compared with the middle group whose lifetime exposure was 36 to 40 years. This suggests other factors may be involved in women whose menopause is significantly delayed.
Insulin resistance
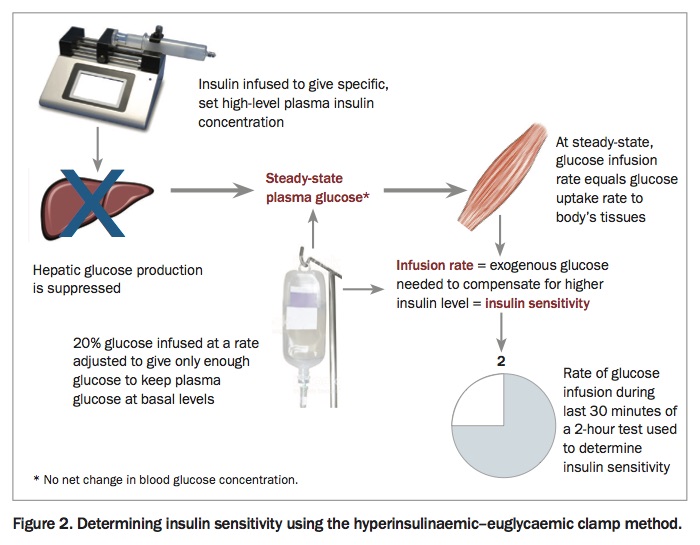
Increased insulin resistance is readily detectable in ovariectomised mice. This effect seems to be mediated by decreased estradiol action on the oestrogen receptor alpha of skeletal muscle, macrophages and adipose tissue, as well as hepatic effects that can lead to hepatic steatosis.9 However, as already noted, studies in women have been less conclusive. Studies using the hyperinsulinaemic–euglycaemic clamp method to measure insulin sensitivity (Figure 2) generally show no difference in insulin action between pre- and early postmenopausal women after adjustment for fat-free mass.15
{kind=link}
One possible explanation for these differing results may be related to how estradiol is synthesised. In postmenopausal women estradiol is synthesised in extragonadal sites such as breast, bone, muscle and adipose tissue where it exerts local paracrine or intracrine effects. Peripheral estradiol actions in postmenopausal women depend on its biosynthesis from circulating adrenal androgens. In rodent models, which are usually ovariectomised, the circulating source of ovarian androgens is suppressed. This means that the adrenal glands do not produce androgens, which results in a much more severe cellular oestrogen deficiency than that found in postmenopausal women.16
Effects of MHT on type 2 diabetes risk
Most studies on postmenopausal women have focussed on cardiovascular disease and coronary heart disease. Although diabetes and metabolic disease are surrogate markers for cardiovascular disease and coronary heart disease, there is a dearth of MHT studies in postmenopausal women where diabetes is a primary endpoint. The results relating to diabetes in these studies have mostly been positive, although several studies have reported increased post-challenge glucose concentrations despite reporting lower fasting glucose levels among MHT users.
In a meta-analysis of 107 trials comparing MHT with placebo or no treatment in postmenopausal women, MHT was associated with a reduction in both fasting glucose and insulin levels, which led to a 13% reduction in insulin resistance and an estimated 30% reduction in new onset diabetes in the MHT group versus the placebo group.7 The first major RCT to examine the relationship between MHT and diabetes was the Postmenopausal Estrogen/Progestin Interventions (PEPI) study.3 This trial reported a significant decrease in both fasting glucose and insulin levels in MHT users versus controls. The Heart and Estrogen Replacement Study (HERS), a RCT of women with established cardiovascular disease receiving MHT or placebo, reported a 35% reduction in diabetes over four years in the treatment group compared with those taking placebo (HR, 0.65; 95% CI, 0.48–0.89). This effect was thought to be due to the lower fasting glucose levels.4
The most recent data come from the Women’s Health Initiative RCT.6 Investigators examined the incidence of diabetes through self-reported treatment with either insulin or oral antidiabetes agents. After one year, lower fasting glucose and insulin levels were seen in the MHT arm compared with the placebo arm. After 5.6 years of follow up, this translated into a statistically significant 21% reduction in incident treated diabetes (HR, 0.79; 95% CI, 0.67–0.93). Interestingly, the protective effect expected of oestrogen was slightly less in the oestrogen only arm of this study compared with participants receiving oestrogen plus medroxyprogesterone acetate.17 In the extended follow up of this study, the beneficial effects of oestrogen (in this case conjugated estrogens) dissipated over time in those participants who ceased MHT, as expected.
The effect of MHT on fasting glucose and insulin levels seen in both the Heart and Estrogen Replacement and the Women’s Health Initiative studies were independent of any reduction in body mass index (BMI). This suggests that MHT has a direct beneficial effect on glucose homeostasis that is independent of fat mass.
The results from these RCTs confirm the findings seen in the following major observational studies.
- The Nurses’ Health Study, an observational study of 21,028 participants followed for 12 years, showed a 20% reduction in diabetes for current compared to past users of MHT after adjustment for age and BMI (HR, 0.80; 95% CI, 0.67–0.96).18
- A prospective French cohort of 63,624 postmenopausal women found a reduced risk of new-onset diabetes among users of MHT after correction for age and BMI (HR, 0.82; 95% CI, 0.72–0.93).19
- A Finnish cohort study of 8483 postmenopausal women who were free of diabetes at recruitment found the adjusted hazard ratio for MHT users versus nonusers after five years was 0.31 (95% CI, 0.16–0.60).20
Effect of mode of delivery on diabetes risk
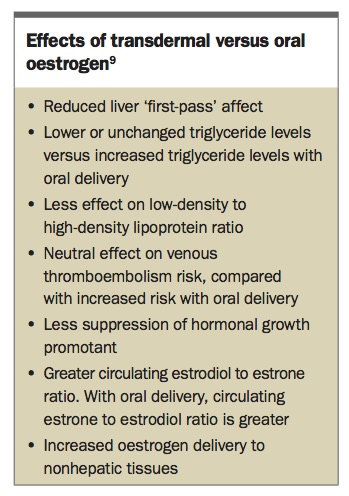
Much of the research on MHT and diabetes risk has been performed using oral oestrogens, either conjugated estrogens or estradiol. However, a growing awareness of the increased thromboembolic risk associated with oral oestrogens has led to a greater use of transdermal estradiol either as a patch or a gel. Transdermal estradiol avoids first-pass liver metabolism and offers a more physiological delivery of hormone into the circulation without adverse side effects such as increased triglycerides, clotting factors and inflammatory markers.21 However, the effects of transdermal estradiol on glucose homeostasis are less than those seen with oral oestrogens. This is probably related to the first-pass effect of oral oestrogens on liver metabolism, leading to a greater suppression of hepatic glucose production. Transdermal oestrogen has a neutral effect on triglycerides, clotting factors and pro-inflammatory markers and delivers more oestrogen to nonhepatic tissues. The ultimate decision on which route of administration of oestrogen is most suitable for the individual woman must therefore be made after assessing her personal needs and risk factors. The different effects between the two modes of delivery are outlined in the Box.9
{kind=link}
Effect of MHT hormones on type 2 diabetes
Oestrogens
MHT has been shown to improve blood sugar control in postmenopausal women with diabetes. A RCT of oral oestrogen in postmenopausal women with diabetes found a decrease in HbA1c level and significant suppression of hepatic glucose production compared with the control group.22 Meanwhile, studies in postmenopausal women taking either conjugated estrogens or estradiol showed reduced fasting glucose and HbA1c levels and less insulin resistance in those taking the oestrogens versus those taking placebo.23,24 It should be noted that these studies were smaller and shorter than the studies following women without diabetes.
Progestogens
Most studies of MHT and diabetes have shown that the beneficial effects of oestrogen on carbohydrate metabolism are attenuated by the addition of progestogens.7 Most of these studies, including the major RCTs, used a synthetic progestin, medroxyprogesterone acetate. This progestin has glucocorticoid activity and has been shown to reduce the beneficial effects of oral or transdermal oestrogens on insulin resistance and cardiovascular risk. Similar effects have been seen with progestins that bind to androgen receptors, although these effects are dose related and not seen, for example, with low-dose norethisterone. In contrast, nonandrogenic progestogens have less adverse effects. Both the retro progesterone, dydrogesterone, and micronised progesterone have been shown to only weakly attenuate the beneficial effects of oestrogens on glucose homeostasis.21,25
Mechanisms of action
Although it has been a commonly held belief that oestrogen improves glucose homeostasis by reducing abdominal fat, data from major RCTs show the effect of oestrogens on the incidence of diabetes is independent of a reduction in BMI. The most likely mechanism of action is a direct effect on oestrogen receptors in fat, muscle and liver, which improves insulin sensitivity. An effect on oestrogen receptors in the pancreas leading to improved insulin secretion is also a possibility.26 A meta-analysis has shown MHT leads to improvements in the insulin resistance homeostasis model assessment, or HOMA-IR, that lends support to these hypotheses.7
Hyperinsulinaemic–euglycaemic clamp studies in women have shown no beneficial effect of MHT on insulin action,9 which suggests exogenous oestrogen may improve glucose homeostasis independent of any direct insulin action. As noted earlier, several studies have demonstrated that conjugated estrogens alone or in combination with medroxyprogesterone acetate decrease total and intra-abdominal fat, most likely by increasing lipid oxidation and energy expenditure.27 RCTs in postmenopausal women have also shown that MHT may reduce diabetes by promoting suppression of hepatic glucose production.9
Risks-benefits of MHT treatment
It is important to note that the effect of MHT on diabetes has not been a primary endpoint in any of the major RCTs mentioned. The balance between risks and benefits of MHT remain complex. For this reason, and because it remains unclear exactly how oestrogen exerts these beneficial effects, MHT is not recommended as a primary treatment for type 2 diabetes or its prevention. The primary indication of MHT is alleviation of menopausal symptoms. There is a vast body of evidence, accumulated over decades, that clearly demonstrates that when used appropriately in women within 10 years of their last menstrual period, MHT also has beneficial effects on bone and cardiovascular health.
A useful guide for clinicians wishing to use MHT, particularly if they are not familiar with recent guidelines and position statements, may be found in the A Practitioner’s Toolkit for the Management of the Menopause.28,29 These algorithms and supporting text are designed for desk top use and endorsed by the International Menopause Society, the Australasian Menopause Society and the Jean Hailes Foundation.
Risks–benefits considerations of MHT for diabetes
Based on the clinical trial evidence to date, it is possible to draw the following conclusions to help assess the risks and benefits involved in prescribing MHT to an individual.
Within 10 years of menopause and no diabetes
For women within 10 years of their menopause there is good quality evidence that the benefits of MHT greatly outweigh any risks. For those in this group who:25
- have undergone a hysterectomy, oestrogen-only MHT may reduce the risk of type 2 diabetes and coronary heart disease
- have an intact uterus, using combined oestrogen plus progestogen therapy may also be a benefit, although synthetic progestins particularly attenuate this effect.
With type 2 diabetes and transitioning into menopause
Women with type 2 diabetes undergoing the transition into menopause may experience an improvement in glucose homeostasis with oestrogen therapy, again attenuated if a progestogen is required. Diabetes is regarded as a risk factor for coronary heart disease. Because of the neutral to beneficial effects of oestrogen on glucose homeostasis, in the absence of other risk factors, MHT, if indicated, may be used in this population.25
Other MHT risk factors
A thorough risk assessment should be performed before initiating MHT in women who:25
- are obese
- have increased risk factors for cardiovascular disease
- are older than 60 years
- have not had a period in over 10 years.
If suitable for MHT, these women should be prescribed nonoral oestrogen plus a neutral progestogen.25
Conclusion
Despite some uncertainty surrounding the exact mode of action, RCTs in postmenopausal women suggest that the incidence of type 2 diabetes may be adversely affected by the age at which menopause occurs and by several factors linked to the menopause, including changes in body fat distribution and glucose homeostasis. Various guidelines, recommendations and position statements all conclude that MHT may be effective in reducing the incidence of new cases of type 2 diabetes in postmenopausal women but stop short of recommending MHT for prevention of postmenopausal type 2 diabetes.24,30,31 Limited evidence also suggests that glucose homeostasis might be improved in women with pre-existing type 2 diabetes who have chosen to take MHT to alleviate their menopausal symptoms as they undergo the transition into menopause. ET
Dr Phua: None.