A routine ECG during a routine health check

Heart diseases
Emergency medical services
Routine ECG testing is increasingly common in current medical practice. Being aware of a wide differential for abnormalities is an important part of current practice.
As a general practitioner working in your own practice and the local emergency department, you review many ECGs. The detection of asymptomatic ECG abnormalities during routine health checks, including those initiated by employers, can lead to referral to the local emergency department, as illustrated by the case discussed below.
The case
You are working on a busy evening shift in the emergency department when you hear an announcement from triage that there is a category 2 case (urgent, must be seen within 10 minutes) coming into the acute area. A 34-year-old businessman was having a two-yearly exercise stress test as part of an employer-initiated health assessment when it was noted that his pre-exercise ECG was abnormal. The test was terminated and he was referred to the emergency department. He has self-presented and tells you that he has had ‘no symptoms whatsoever’ apart from being a bit more tired than usual, which he had put down to long hours at work. On thorough questioning he reports a decreased exercise tolerance.
The patient’s referral letter states that the resting ECG shows abnormalities that were not present in ECGs performed two years ago. The triage nurse notes that the patient is pain free.
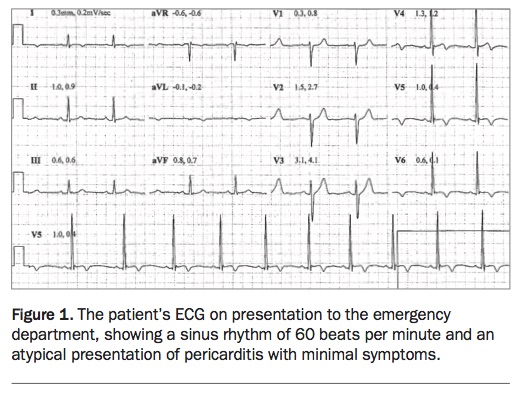
Despite knowing that in most similar cases the ECG abnormalities are due to lead placement, your team follows standard protocol and the patient is immediately moved to an acute bed and placed on cardiac monitoring. An initial ECG is performed, which confirms the changes seen as an outpatient (Figure 1). An intravenous cannula is inserted and initial blood tests are taken and a chest x-ray ordered.
{kind=link}
The history
The patient, an engaging man, said that he attended the health assessment clinic as part of a routine program that his employer requires to adjust company-wide life insurance premiums. He is understandably concerned that there is something wrong with his heart. He had a similar health review two years ago and was told then that his cholesterol level was mildly elevated, especially his LDL-cholesterol level, and was advised to change his diet to attempt to lower it. He has since stopped drinking coconut water and switched to margarine and low-fat dietary alternatives.
The patient initially denies any symptoms, including chest pain. On closer questioning he noted that he has been very short of breath since getting the ‘man flu’ two weeks ago. His respiratory illness was characterised by coryzal symptoms, subjective fevers, severe myalgias and fatigue. Since then he has had shortness of breath on routine exercise and felt very tired. He spent the past weekend sleeping on the couch, which was very unusual for him. He had assumed this was due to a busy work schedule. He has had no ankle swelling or other signs of heart failure. He travelled to Korea about six weeks ago. He denies any rural travel, mosquito or insect bites, tattoos, intravenous drug use or sexual encounters overseas. He has no known sick contacts.
He has no past history of heart disease, renal disease, hypertension or diabetes and is a nonsmoker. He drinks on the weekend but does not use illicit drugs, including amphetamines or anabolic steroids. His family history includes a paternal grandfather with a heart attack in his 70s, but no other significant cardiac disease. He takes no prescribed medications. During his recent respiratory illness, he took paracetamol, ibuprofen and over-the-counter cold and flu medications that contained pseudoephedrine hydrochloride and codeine phosphate. He has an active lifestyle and exercises regularly two to three times per week.
Physical examination
On examination, the patient has no abnormalities detected on cardiovascular or respiratory examination.
Test results and provisional diagnosis
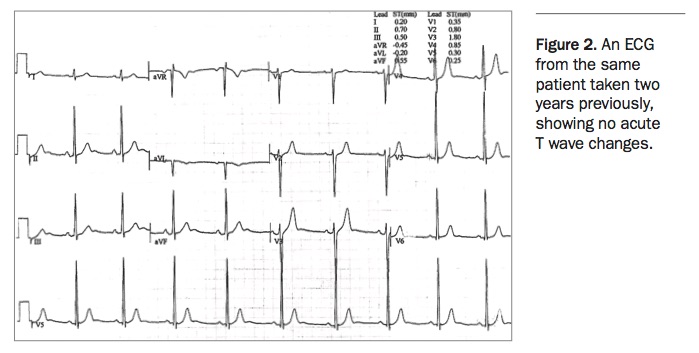
On analysing the ECG (Figure 1), you immediately note sinus rhythm at 60 beats per minute. The axis is within normal limits. There is T wave inversion in leads I, AVL and V4 to 6. There is also PR depression in leads II, AVF and V1 to 6, more pronounced in lateral chest leads. You compare this with an ECG taken two years previously (Figure 2), which shows sinus rhythm with no acute changes.
{kind=link}
The patient’s blood tests, including troponin level, and chest x-ray show no abnormalities.
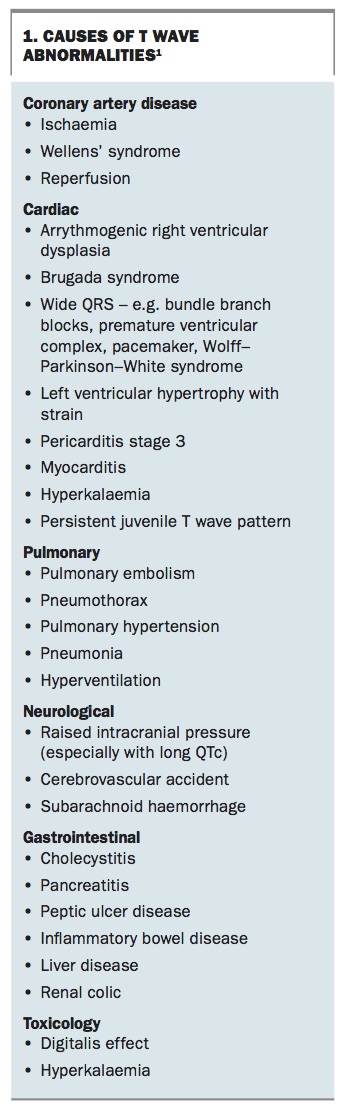
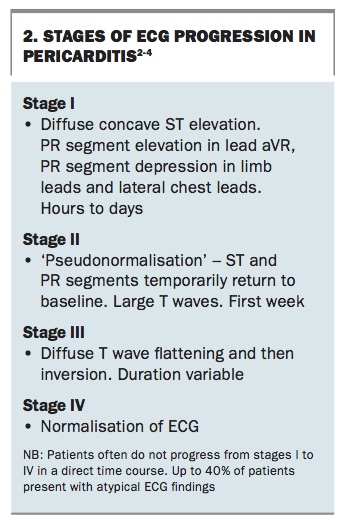
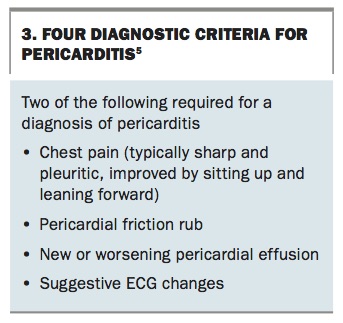
Based on the history and ECG, you are concerned this patient may have pericarditis. Box 1, Box 2 and Box 3 list the causes of T wave abnormalities, the stages of ECG progression in pericarditis and diagnostic criteria for pericarditis.1-5
{kind=link}
{kind=link}
{kind=link}
Management
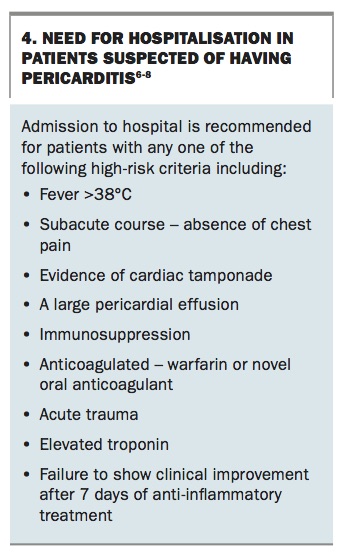
You immediately discuss the case with the cardiology department, and it is agreed the patient should be seen in rooms early the next morning. You reassure the patient and discharge him after a single dose of oral colchicine 0.6 mg. The need for hospitalisation in patients suspected of having pericarditis is discussed in Box 4.6-8
{kind=link}
You later follow up with the cardiologist to find that a transthoracic echocardiogram showed normal left ventricular wall motion and ejection fraction, with a small amount of scarring on the posterior wall of the left ventricle but no pericardial effusion or impairment in left ventricular ejection fraction. The ECG changes had already resolved by presentation to the cardiologist.
After discussion with the cardiologist, it was agreed to cease the colchicine because of the lack of symptoms or findings. The patient was discharged from cardiology care with no further medication or follow up. He was advised to avoid strenuous exercise for four weeks (i.e. nothing more severe than walking at a speed he could hold a conversation).
Discussion
Pericarditis is a common disease and in developed countries is most commonly assumed to be caused by viruses.6,9 It is particularly important to be mindful of pericarditis during outbreaks of influenza and viral gastroenteritis. Rarely pericarditis can represent the first symptom of an autoimmune or malignant disease. Pericarditis and associated myocarditis can result in long-term complications including pericardial effusion and tamponade or heart failure.
Routine ECG testing is increasingly common in current medical practice. Being aware of a wide differential for abnormalities is an important part of current practice, as clinicians are the frontline in detecting cardiac disease.
It is interesting to reflect on the utility of ‘routine executive health checks’. There are many arguments against the use of investigations without a clinical question, including how the interpretation of abnormal results without clinical symptoms, overservicing, potential harms from follow- up investigations and treatment of illness that would not have caused morbidity or mortality. ‘General health checks did not reduce morbidity or mortality, neither overall nor for cardiovascular or cancer causes, although the number of new diagnoses was increased.’10 However, it is important to ask whether there is also some benefit. In the discussed case, did the detection of incidental ECG changes alter management? Quite possibly. Although the authors do not recommend such investigations, this patient was able to avoid strenuous exercise and avoid any potential long-term complications of pericarditis. MT