Childhood weight issues. Seeking better health outcomes

Obesity in children
Children's health
Most children and adolescents who are overweight or have obesity are identified through primary health care. The role of a GP in assessing and managing this population is integral in optimising the health of these young people and improving their psychosocial outcomes. This article outlines an approach for primary clinicians to follow when they encounter a child or adolescent with overweight or obesity.
- GPs are well positioned to identify overweight and obesity in children and adolescents.
- Raising the issue can be difficult but it is often well received.
- Simple strategies such as routine monitoring of body mass index in addition to targeted history taking and physical examination can assist in assessment.
- Brief, opportunistic interventions, including advice about the benefits of weight loss, have proven effective.
- Management strategies should be family-based and consist of lifestyle interventions as well as supportive measures for behavioural change.
- Early intervention leads to better outcomes.
Although the prevalence of paediatric overweight and obesity seems to have plateaued over the past five to 10 years, it still remains high with one in four Australians aged 5 to 17 years above a healthy weight range.1 However, the prevalence of severe obesity is increasing, as is the prevalence among certain cohorts, including older adolescents and pre-schoolers, as well as those from lower socioeconomic areas.1 Furthermore, there has been a significant increase in abdominal obesity.2 Children and adolescents with obesity, and even overweight, are at an increased risk of weight-related complications including, but not limited to, type 2 diabetes, hypertension, joint issues, obstructive sleep apnoea, fatty liver disease and significant psychosocial morbidities. The good news is that complications are reversible if addressed early.
Children with obesity present to healthcare services more often than those within the healthy weight range, and the total healthcare costs of children with obesity are 1.62 times those of children with a healthy weight, even at the young age of 2 to 5 years.3 Therefore, it is essential to identify early those children at risk or already affected by obesity. Addressing this issue requires a multifaceted approach. There should be a focus on prevention of unhealthy weight gain by encouraging family-wide lifestyle modifications in relation to healthy eating and physical activity, as well as supporting behavioural change.4 The Clinical Practice Guidelines for the Management of Overweight and Obesity in Adults, Adolescents and Children in Australia from the NHMRC recommend the ‘5 As’ approach to the management of obesity: ask, assess, advise, assist and arrange.4
Ask
Recognising and raising the issue is often the biggest barrier to commencing interventions to improve the health of a child with overweight or obesity. Although weight may be a sensitive topic for young people and their parents, studies within the primary care setting suggest that raising the issue with patients is often well received, and in fact expected, and interventions offered by GPs are deemed appropriate and helpful rather than offensive.5,6 Often the patient is attending the GP because of a health issue that may well be exacerbated by obesity, but weight is not the primary concern of the family. To raise weight-related concerns with families, the height and weight of the child or young person can be measured with subsequent plotting of body mass index (BMI) on age- and sex-appropriate centile charts. The child or young person’s growth can then be monitored, the BMI chart can be used to start the conversation about excessive weight gain and interventions can be initiated at the appropriate time. This routine should be made standard practice for all children attending the clinic, not just those who have a perceived excessive weight gain.4,7
The NHMRC guidelines suggest using the World Health Organization charts for children under 2 years of age and the US Centers for Disease Control charts for children and adolescents above 2 years of age. Children and adolescents with a BMI greater than the 85th percentile are classed as overweight and those with a BMI exceeding the 95th percentile fall into the category of obese. Discriminatory or stigmatising language should be avoided. For example, instead of saying ‘an obese child (or person)’ it is better to talk about children with obesity – they are a person first and foremost and have a condition. Discussion should be oriented around the benefits of healthy lifestyle behaviours for the family rather than the weight of the young person.4 It is recommended that when talking with families to speak in terms of ‘above a healthy weight’ for those in the overweight category and ‘well above a healthy weight’ for those in the obese category.
Assess
In addition to regularly plotting BMI on appropriate growth charts, it is recommended that assessment also encompass history taking, clinical examination and relevant investigations to help determine current health problems and risks for future disease and morbidity.4,7 If time is limited or the patient has not initially come in for weight-related concerns, it may be necessary to arrange several short additional appointments to glean the necessary information over time.
History taking
Young people and their parents should be asked if they have any weight-related concerns and if any previous attempts at weight loss have been successful. History taking should include, but is not limited to, assessment of the following areas:
- weight history, including onset and duration of weight gain and its impact on the young person and their family
- potential underlying comorbidities, for example:
– obstructive sleep apnoea (ask about nocturnal enuresis,
snoring, witnessed apnoeas, morning headaches,
daytime somnolence)
– respiratory problems (ask about exacerbation of asthma,
exercise tolerance levels)
– other systemic problems (ask about constipation,
gastro-oesophageal reflux and orthopaedic concerns such
as back and joint pain)
– psychosocial or behavioural problems (ask about bullying,
school refusal, depression, attention deficit hyperactivity
disorder and autism spectrum disorder, all of which have
an increased prevalence in children with obesity)
- family history of obesity, bariatric surgery or cardiometabolic problems such as diabetes and hypertension
- ethnicity (as there is a higher prevalence of obesity and associated comorbidities in people of Asian, Middle Eastern, Indigenous Australian and Pacific Islander descent)
- dietary history, including eating patterns of the family, regularity of meals, snack choices, drinking habits and consumption of fast food
- other lifestyle factors (ask about screen time, level of physical activity, both organised and incidental).
Physical examination
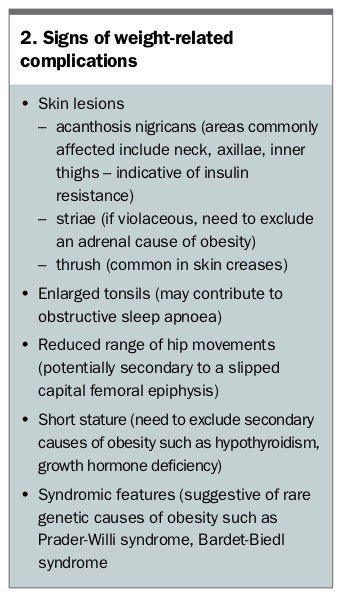
In addition to BMI, waist circumference should be measured to calculate waist-to-height ratio (Box 1). This gives a more accurate indication of fatty tissue distribution and risk than either BMI or waist circumference alone. A waist-to-height ratio of more than 0.5 is associated with increased cardiometabolic risk.2 Blood pressure should also be measured with an appropriately sized cuff. Some signs of weight-related complications to look for during examination are listed in Box 2.
{kind=link}
{kind=link}
Investigations
Most children with overweight or mild obesity do not require further investigations. However, they may be warranted in older adolescents, those with extreme obesity, those with a significant family history of obesity or related complications, those in whom the physical examination is suggestive of comorbidities, and patients with short stature. If blood tests are required, it is recommended that they are performed fasting and include the following: liver function tests, iron studies, measurement of glucose and insulin levels, a lipid profile and vitamin D level. Although underlying medical causes of childhood obesity are rare, it is important to exclude conditions such as Cushing’s syndrome, hypothyroidism, growth hormone deficiency and hypopituitarism/hypothalamic disorders if the history or examination flag these as possible concerns and to arrange investigations where indicated. For example, thyroid function tests should be considered in patients with short stature or when height trajectory reduces unexpectedly. Patients with a history suggestive of obstructive sleep apnoea should be referred for a sleep assessment. If obtaining a fasting blood sample is a challenge then HbA1c may be measured as a minimum to exclude type 2 diabetes.
Advise and assist
Opportunities are being missed for timely intervention in childhood obesity.8 Barriers to action include insufficient time and resources and a lack of belief in the effectiveness of interventions. Evidence is, however, accumulating for the effectiveness of lifestyle intervention in paediatric obesity in the short term with a new series of six Cochrane reviews about childhood obesity.9-14 More evidence is needed for longer-term outcomes.
An intervention trial of 76 children aged 5 to 16 years, in which the families were offered five appointments over 12 months, demonstrated that outcomes in the GP setting were as good as those in the tertiary setting (mean BMI standard deviation score reduced by 0.17 in the GP setting compared with 0.15 in the tertiary setting).15 In adults with obesity, a randomised controlled trial demonstrated the efficacy of a brief, 30-second, opportunistic intervention implemented by primary care physicians.5 This type of intervention may not be generalisable to the paediatric population but does demonstrate that not much time is required to achieve a positive result.
Given the proven benefits of providing advice and support for weight loss, young people and their families should be counselled on the benefits of weight management. The importance of a family-based approach cannot be overstated. Family-wide behaviour change will lead to better outcomes and more successful lifestyle changes in children and adolescents.4,15 The early development of positive lifestyle behaviours can contribute to reducing the risk of shorter-term, obesity-related complications while preventing longer-term comorbidities such as diabetes, cardiovascular disease and mental health issues in adulthood.
The use of multicomponent lifestyle interventions for the management of overweight and obesity in children and adolescents is encouraged. In most children the aim is to be weight stable while they grow in height. However, in children and adolescents with severe obesity, weight loss will most likely be required to reduce comorbidities. Interventions usually include a combination of more age-appropriate or reduced energy intake, reduced sedentary behaviour (particularly reduced screen time), increased physical activity (especially incidental), improved sleep routines and measures to support behavioural change including family involvement. Further referral may be required (see below).
‘SMARTER’ goal and motivational interviewing techniques can be used to identify problem areas and help clarify goals. ‘SMARTER’ goals are specific, measurable, achievable, relative, timely and associated with an emotion and reward.7 For example, although implementation of interventions is carried out through working with the parents as agents of change, to help gain the child’s cooperation you could talk about how exciting (the emotion) it will be for the child to choose what activity the family does over the weekend (the reward) when the weekly goal is reached. Suggestions for family activities include going cycling or having a picnic in the park. Ideally, rewards should not be specific food or screen related and should be commensurate with the aims. Small stepwise changes are often easier to implement and usually more sustainable. Frequent contact with a healthcare professional allows for regular monitoring and feedback. This provides accountability and is associated with improved outcomes of weight management interventions.4,7 Suggestions for simple interventions are listed in Box 3.
{kind=link}
Arrange
Referral of the patient to local dietetic, physio-therapy and clinical psychology services is likely to assist in improving health outcomes. Free community programs can be accessed within NSW, including Go4Fun (a 10-week healthy lifestyle program tailored to children aged 7 to 13 years) and Get Healthy (a service aimed at adolescents aged 16 years and older and their carers). Specific community interventions in other states and territories are very limited except in Western Australia, where The Better Health Company runs a program similar to Go4Fun.
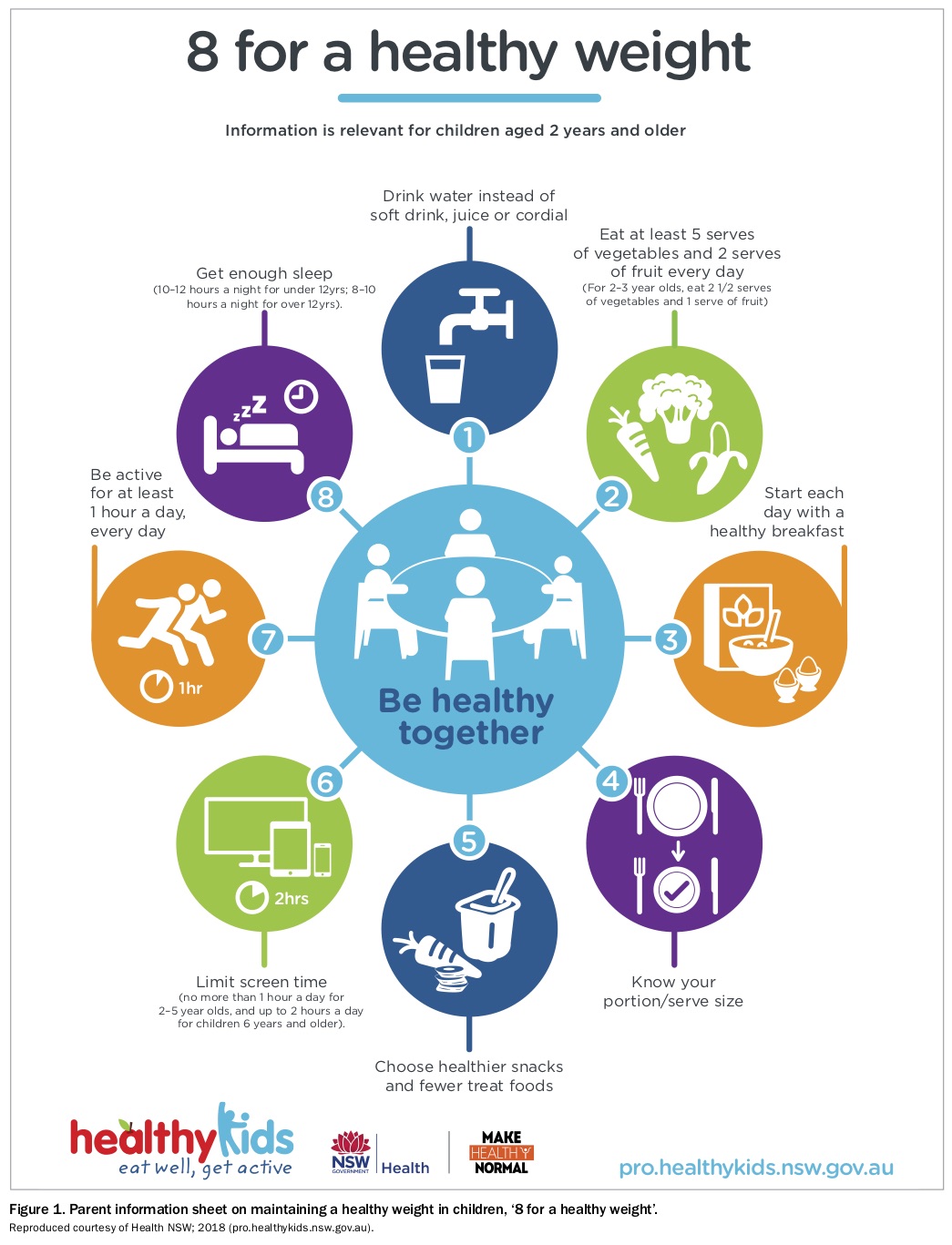
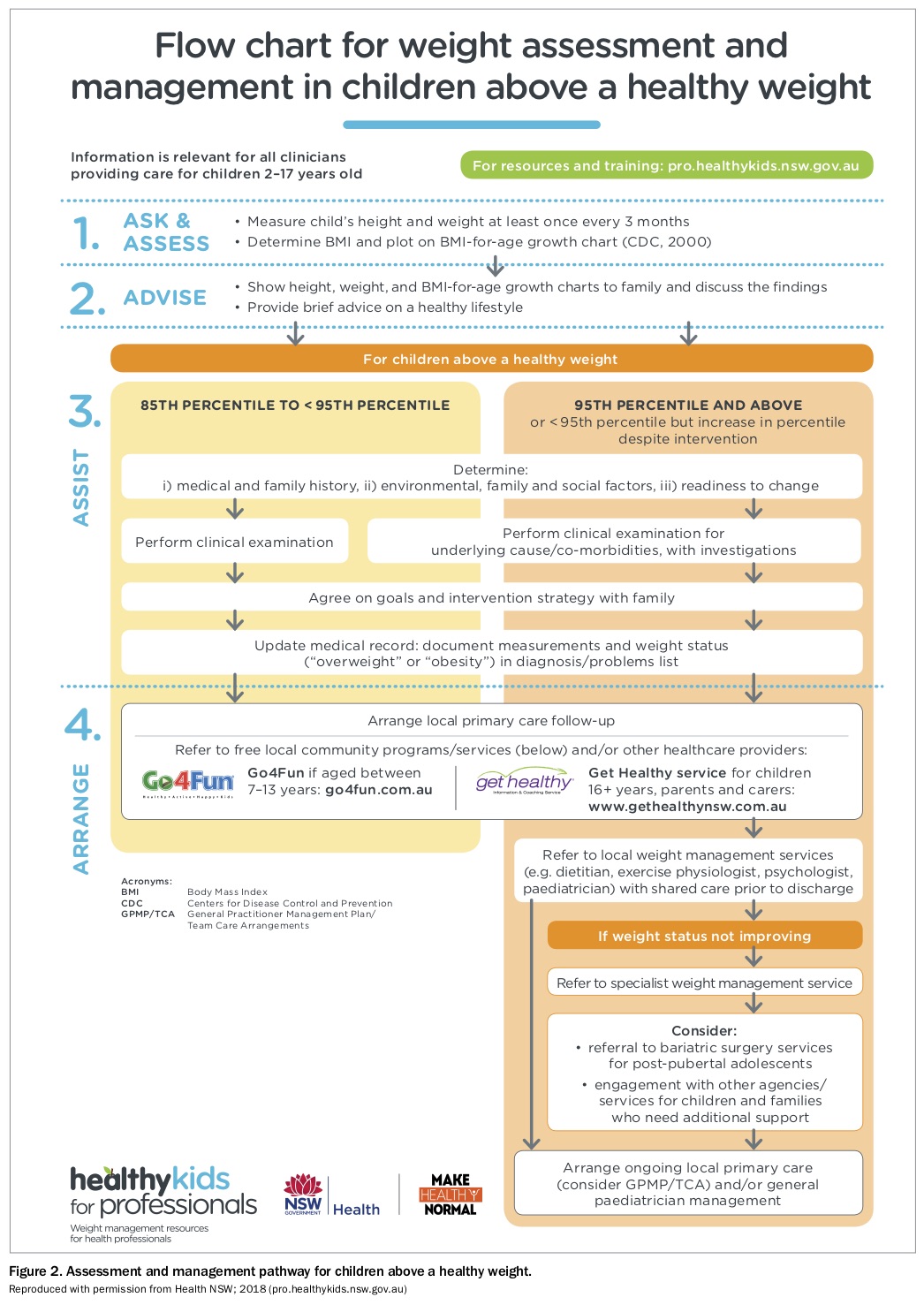
A new ‘one-stop shop’ website for healthcare professionals, Healthy Kids for Professionals (pro.healthykids.nsw.gov.au), has been developed through a collaboration between the NSW Ministry of Health and a working group on paediatric obesity. Several resources have been developed and can be accessed via this website, including video vignettes on how to start the conversation, the parent information sheet ‘8 for a healthy weight’ (Figure 1; available in several different languages), weight assessment and management pathways (Figure 2) and referral links to new and existing dietitian-led or multidisciplinary clinics within NSW. An online learning program for healthcare professionals, Weight4KIDS, can also be accessed via the Healthy Kids website. Another online learning program, Talking with Parents About Children’s Weight, is available via the Better Health Company’s website (Box 4).
{kind=link}
{kind=link}
{kind=link}
For patients with severe obesity and associated comorbidities, specialist referral to a paediatrician or multidisciplinary weight management team may be required. This should be considered when:
- BMI is greater than 99th centile for age
- there is no change in BMI centiles or in symptoms of existing conditions despite improvement in health behaviours
- new comorbidities are identified
- there are multiple comorbidities.
Medication interventions (metformin [off-label use for obesity] and orlistat) are limited and should only be used in conjunction with lifestyle changes. Specific dietary interventions such as very-low-energy diets or intermittent fasting should be done under supervision from a dietitian with expertise in paediatric weight management. Bariatric surgery at present is not readily available within the public sector. Guidelines are available via a joint college statement with consideration being limited to adolescents who are postpubertal (at least 15 years of age) and have a BMI greater than 40 kg/m2 or greater than 35 kg/m2 with comorbidities.4
Conclusion
Early recognition of overweight and obesity in children and adolescents leads to early intervention with better health and psychosocial outcomes. Taking an opportunistic, family-based approach to managing young people with weight-related issues is encouraged. The use of a simple, structured strategy similar to that outlined above will assist in reducing the prevalence of both short- and long-term obesity-related complications and comorbidities in this population group. ET