Postmenopausal osteoporosis: is there a role for menopausal hormone therapy?

Dr Fernandes is a Research Fellow in the Department of Endocrinology and Diabetes, Royal Brisbane and Women’s Hospital. Dr Jang is a Senior Staff Specialist in the Department of Endocrinology and Diabetes, Mater Health Brisbane, and a Senior Lecturer at the University of Queensland, Brisbane. Professor Duncan is a Pre-Eminent Senior Staff Specialist and Consultant Physician in the Department of Endocrinology and Diabetes, Royal Brisbane and Women’s Hospital; Adjunct Professor at the Institute of Health and Biomedical Innovation, Faculty of Health, Queensland University of Technology; and Professor of Medicine at the University of Queensland, Brisbane, Qld.
Osteoporosis
Menopause
Menopausal hormone therapy (MHT) increases bone density and prevents fracture. However, the publication and accompanying media coverage of the Women’s Health Initiative study made many women fearful of MHT and many doctors reluctant to prescribe it. There is increasing recognition that MHT does have a place in health management of postmenopausal women, including for fracture prevention.
- Oestrogen-alone and combined oestrogen–progestogen therapy increase bone mineral density and reduce vertebral and nonvertebral fractures in postmenopausal women.
- Use of menopausal hormone therapy (MHT) in general, and for osteoporosis specifically, has been controversial since the early closure of the Women’s Health Initiative (WHI) study.
- In the final analysis of the WHI study, the benefits of MHT were found to be considerable and, particularly for younger women, may outweigh the risk of harm.
- Commencing MHT is a valid option for postmenopausal women under the age of 60 years and within 10 years of menopause, with no specific contraindications, not only for vasomotor symptoms but also for bone protection.
To paraphrase Professor Bronwyn Stuckey, menopause is a consequence of improved public health: most women now not only survive childbirth but also their childbearing years and live long enough to experience loss of ovarian function (at an average age of 51 years). Menopause is generally rare among mammals, occurring only in humans, short-finned pilot whales and killer whales.1
This article focuses on the use of menopausal hormone therapy (MHT) with respect to bone health and discusses the evidence for combined oestrogen–progestogen therapy, oestrogen-alone therapy in women who have had a hysterectomy, selective oestrogen receptor modulators (SERMs), tissue-selective oestrogen complexes (TSECs), and tibolone. Use of MHT in glucocorticoid-induced osteoporosis, premature or early menopause (cessation of menses before the age of 40 or 45 years, respectively) and functional hypothalamic amenorrhoea (e.g. anorexia nervosa) is not covered.
MHT and bone
Oestrogen
It is hard to overestimate the importance of oestrogen to the skeleton. The rapid rise in bone mineral density (BMD) from increasing levels of gonadal hormones at puberty is predominantly due to oestrogen, in both sexes. Oestrogen secretion causes growth plate closure and thus determines a person’s final height. Oestrogen is important for osteoblasts, osteoclasts and osteocytes and maintains both cortical and trabecular bone.2 It also mediates the skeleton’s response to mechanical loading via sclerostin suppression.3
Oestrogen deficiency causes rapid bone loss at menopause – with greater than 10% of bone mass at the lumbar spine and greater than 9% at the femoral neck being lost in the decade after menopause, mostly in the year before and two years after the final menstrual period – and contributes to ongoing bone loss thereafter.4
The three major endogenous oestrogens in women are oestrone, oestradiol and oestriol, with oestradiol being the most biologically active form. There are multiple pharmacological oestrogen formulations available in Australia, including 17-beta estradiol, combined estrogens and the synthetic oestrogens ethinylestradiol and mestranol. Conjugated equine estrogens (CEEs), originally derived from pregnant mares’ urine, contain various estrogens, with the predominant form being estrone sulfate, which is metabolised to estrone and then estradiol.
Oestrogen binds to nuclear oestrogen receptors (ERs). There are two subtypes (ER-alpha and ER-beta), expressed differently in different tissues, with ER-alpha the predominant ER in cortical bone, breast and endometrium. Upon ligand binding, ERs undergo conformational change and dimerisation, ultimately affecting DNA transcription.2
In the 1970s, the use of oestrogen-alone therapy in women with an intact uterus caused endometrial hyperplasia and increased the risk of endometrial cancer. These complications were almost entirely obviated by the addition of progesterone, particularly if given continuously.5
Intravaginal oestrogen has a theoretical risk of endometrial hyperplasia; however, compared with placebo or baseline incidence rates, no increase in endometrial hyperplasia or carcinoma has been observed at 12 months, using endometrial biopsy or ultrasound, respectively.6,7 Data regarding long-term risks are lacking, but progesterone coadministration is generally thought unnecessary.8
Selective oestrogen receptor modulators and tissue-selective oestrogen complexes
SERMs have oestrogenic effects in some tissues (e.g. bone) but oestrogen-antagonistic effects in others (e.g. breast and uterus). Like oestrogen, SERMs interact with nuclear ERs. The tissue-specific agonist versus antagonist effects of SERMs depend not only on ER subtype distribution and binding, but also on differing compositions of the ER–ligand complex, its dimerisation and conformational change, and the coactivators and/or corepressors available in any particular cell type.9
Two SERMS are available in Australia: raloxifene and bazedoxifene. Lasofoxifene, another SERM, is currently unavailable. At the endometrium, raloxifene has a neutral effect (as does lasofoxifene), whereas bazedoxifene is anti-oestrogenic.10 Thus, bazedoxifene can be coadministered with oestrogen without additional endometrial protection.11
TSEC therapy refers to the combination of a SERM plus oestrogen and is available in Australia as bazedoxifene plus CEE.
Tibolone
Tibolone is a biologically inactive synthetic steroid, but its three active metabolites are weak agonists of the ER (e.g. bone and vaginal tissue), progesterone receptor (e.g. endometrium) and androgen receptor.
Progestogens
Progesterone is the major progestogen in humans and is secreted predominantly by the ovaries, affecting the uterus, vagina, cervix, breasts and brain. Progesterone binds to the progesterone receptor (both nuclear and membrane forms) and to other nonaromatised steroid receptors; namely, androgen, glucocorticoid and mineralocorticoid receptors. For example, progesterone antagonises aldosterone at the mineralocorticoid receptor, altering fluid balance during the menstrual cycle.
There are many progestogens available in Australia. Progesterone itself is available orally as micronised progesterone. Synthetic progestogens (collectively termed progestins) include medroxyprogesterone acetate, etonogestrel, levonorgestrel and norethisterone. Progestogens are also available in combination with oestrogen, in both oral and transdermal formulations. In addition to binding to the progesterone receptor, different progestogens have varying profiles at the other steroid receptors. Thus, side effects differ between agents.
Androgens
Androgens affect the skeleton indirectly (via aromatisation to oestradiol and the ER) and possibly directly (through the androgen receptor).12 In hypogonadal men, the main mechanism by which testosterone prevents bone loss is through conversion of testosterone to oestradiol.13 In women, an independent effect of testosterone on bone remains poorly defined.14
Dehydroepiandrosterone (DHEA) and DHEA-sulfate
Dehydroepiandrosterone (DHEA) is derived predominantly from the adrenal cortex (90%), with only 10% produced by the gonads. DHEA-sulfate (DHEA-S) is produced almost exclusively by the adrenal gland. Both DHEA and DHEA-S can be metabolised to oestrogens and androgens. Their contribution to overall postmenopausal gonadal hormone levels (which are, in any case, low) is not well defined. Whether either has an independent skeletal effect is unknown.
Does MHT improve bone health?
Oestrogen-alone and combined oestrogen–progestogen
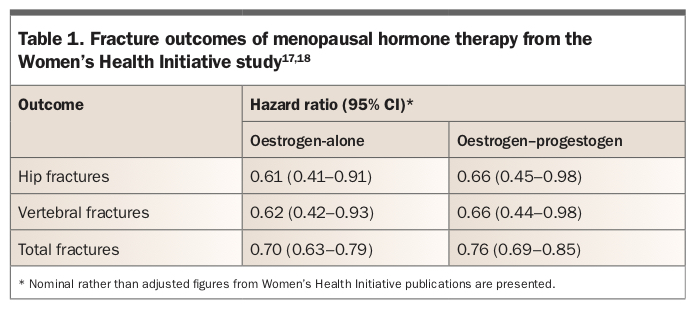
Both oestrogen-alone and combined oestrogen–progestogen therapy improve BMD and prevent vertebral and nonvertebral fractures (including hip fractures) in postmenopausal women.
An early randomised controlled trial showed that oestrogen improved BMD, consistent with observational data showing that it decreased fracture risk.15,16 One of the indisputable findings of the Women’s Health Initiative (WHI) study, involving 27,347 women, was that MHT reduced fracture risk. Compared with placebo, oestrogen-alone reduced hip, clinical vertebral and total fractures by 30 to 39%, and oestrogen–progestogen reduced fractures by 24 to 34% (Table 1).17,18
{kind=link}
MHT may have synergistic effects with calcium and vitamin D on bone health. Some participants in the WHI MHT study also participated in the WHI calcium plus vitamin D study (16,089 women). Women receiving MHT (either oestrogen-alone or oestrogen–progestogen) and calcium plus vitamin D had a nonsignificantly lower risk of hip fracture compared with women taking calcium plus vitamin D but not MHT (hazard ratio [HR], 0.58; 95% confidence interval [CI], 0.37–0.93 vs HR, 1.15; 95% CI, 0.81–1.61; p for interaction, 0.07).19 Within the group of women taking MHT, the comparison of those who did or did not take calcium plus vitamin D is not available.
Although small trials have shown that intravaginal oestrogen improves BMD, fracture data are lacking.20,21 Intravaginal oestrogen is not recommended for bone health.
Do oestrogen and oestrogen–progestogen benefit all postmenopausal women or only those at highest risk of fracture?
The WHI study population was unusually healthy from a bone perspective; hip fracture rates in the placebo group were about 50% lower than expected for an age-matched cohort.22 Nonetheless, a reduction in all fracture types was observed in both study arms. BMD was only measured in 5.7% of participants, and this subgroup was not thought to be representative of the cohort overall. Thus, the capacity of the WHI to assess who best to target for fracture prevention (women with low BMD and osteoporosis or osteopenia, women with other clinical risk factors for fracture, or all postmenopausal women) is limited.
In the oestrogen-alone arm, ‘the effect of CEE on hip and total fractures was remarkably consistent, almost irrespective of individual characteristics’.23 A summary fracture risk score (including age, current smoking status, body mass index and previous fracture, but not BMD) was calculated. There was significant interaction between this score and total fracture risk reduction, such that those with the highest fracture risk score had the greatest reduction in total fracture risk (high risk: HR, 0.66; moderate risk: HR, 0.68; lowest risk: HR, 0.86; p for interaction, 0.04). A similar but nonsignificant trend was observed for risk of hip fracture specifically. Total hip BMD was measured at baseline in 938 women: 5.7% had a T-score less than –2.5 and 38.7% had a T-score between –1 and –2.5. Within this small group, total fracture risk reduction with CEE was insignificant (49 fractures with CEE vs 64 with placebo; HR, 0.77), and no significant interaction of fracture risk reduction with BMD was observed (osteoporotic group: HR, 0.83; osteopenic group: HR, 0.83; women with normal BMD: HR, 0.99; p for interaction, 0.17).23
In the combined oestrogen–progesterone arm, similar but not identical analyses were performed. Reduction in risk of hip fracture was observed regardless of baseline characteristics, with the single exception that reduction in hip fracture risk was only observed in women with a daily calcium intake greater than 1200 mg.24 No interaction was seen between the summary fracture risk score and either hip fracture or total fracture risk reduction. Total hip BMD was measured in 1024 women, and women with a T-score less than –3.0 were excluded from participation. The risk reduction for all fractures in women with a T-score less than –2.5 was 0.53 (with a CI crossing 1; no formal p value was presented), compared with 0.87 in the group with BMD greater than –2.5 (p for interaction of fracture reduction with BMD, 0.15). It is unclear how many women overall had a T-score less than –2.5, and the fracture numbers were small (e.g. 11 fractures with combined oestrogen–progesterone vs 22 with placebo in the low BMD group).24
In extracting meaning from these results, even if the relative risk reduction is the same across the population, the absolute reduction in fractures will be greatest in the group with the highest fracture rate.
SERMs and TSECs
SERMs improve BMD and prevent vertebral fracture. Among 6828 women in the Multiple Outcomes of Raloxifene Evaluation (MORE) trial, raloxifene improved BMD at the femoral neck and spine and reduced vertebral fractures (relative risk, 0.7; 95% CI, 0.5–0.8, p=0.05).25 However, it had no effect on nonvertebral fractures (relative risk, 0.9; 95% CI, 0.8–1.1; p=0.24) or hip fractures (relative risk, 1.1; 95% CI, 0.6–1.9; p=0.71).25 Bazedoxifene has similar efficacy to raloxifene in terms of BMD increases at the hip and spine and vertebral fracture prevention.26 In contrast, lasofoxifene reduces both vertebral and nonvertebral fractures.27
TSECs may be more effective for osteoporosis prevention than SERMs alone. The Selective Estrogen Menopause and Response to Therapy (SMART-1) trial found greater BMD gains at the lumbar spine and hip with a TSEC (bazedoxifene plus CEE) compared with either raloxifene alone or placebo, although this study was not adequately powered for fracture comparison.28
Tibolone
Tibolone prevents bone loss, increases BMD and prevents fracture.29-31 The Long-Term Intervention on Fractures with Tibolone (LIFT) study, involving 4538 women, showed that tibolone significantly reduced vertebral fractures (HR, 0.55; 95% CI, 0.41–0.74; p<0.001) and nonvertebral fractures (HR, 0.74; 95% CI, 0.58–0.93; p=0.01), compared with placebo.29
Isolated progestogen
Whether progesterone has a direct skeletal effect is unresolved.32 The isolated use of progestogens (including transdermal preparations from compounding pharmacies) to prevent or treat osteoporosis is of unproven benefit. Supraphysiological doses, as are used in progestin-only contraceptives, are associated with bone loss (through hypogonadotrophic hypogonadism and secondary oestrogen deficiency), although this appears to be reversible, and increased fracture risk has not been reported.33,34 High-dose progestogens may also stimulate glucocorticoid receptors.32 At lower doses, progestogens may act synergistically with oestrogen: combined oestrogen–progestogen increases BMD about 1% more than oestrogen-alone.35 This difference is statistically significant, but whether it is clinically meaningful is debatable.
Androgens
Although some multivariate analyses suggest an independent effect of testosterone on BMD and fracture risk in women,12 parsing unique and independent effects of individual sex steroids is difficult, even in an experimental setting. Moreover, testosterone does not consistently improve BMD, even allowing for its aromatisation to oestradiol.36,37 Data regarding fracture outcomes and cardiovascular safety are lacking. Testosterone is not recommended for treating postmenopausal osteoporosis.
DHEA and DHEA-S
In ovariectomised mice, DHEA-S showed some oestrogen-independent effects preventing bone loss.38 The clinical relevance of this finding for humans is unclear. A recent multivariate analysis suggested that DHEA-S levels correlated with BMD in both men and women, but this study did not adjust for other sex hormones, including oestrogen.39 Robust evidence that DHEA or DHEA-S independently improves BMD or reduces fracture risk is lacking.36
How does MHT compare with other options for treating osteoporosis?
Pharmacological management of postmenopausal osteoporosis was presented recently in a US Endocrine Society clinical practice guideline.40 A meta-analysis of pharmacological therapy in postmenopausal women (107 trials involving 193,987 postmenopausal women) found that MHT (oestrogen-alone vs oestrogen–progestogen), bazedoxifene, raloxifene, lasofoxifene, tibolone, bisphosphonates, teriparatide and denosumab are all effective treatments for osteoporosis.
All forms of MHT are effective in preventing vertebral fractures. Oestrogen and oestrogen–progestogen are effective for preventing hip fractures, whereas neither SERMs nor tibolone are effective for this outcome.41 Most pivotal trials of bisphosphonates, denosumab and SERMs are in older postmenopausal women; trials in younger postmenopausal women have usually assessed BMD rather than fracture as the primary outcome.42,43
There are few head-to-head studies comparing MHT with other treatments for osteoporosis, whether assessing BMD or fracture, and entry criteria differ considerably between trials. A study in young postmenopausal women aged 45 to 59 years found similar increases in BMD with alendronate versus combined oestrogen–medroxyprogesterone acetate.43 In contrast, a study of older postmenopausal women (aged 65 to 90 years) found greater increases in BMD with alendronate compared with oestrogen (with or without medroxyprogesterone).44 Neither study assessed fracture risk. In considering MHT versus bisphosphonates, bone loss will restart promptly after cessation of MHT, whereas the effect of bisphosphonates may persist after cessation (the duration of persistence varies with different compounds).45
Combination treatment
Trials combining MHT with bisphosphonate therapy have produced contradictory results.44,46,47 A small study of 331 postmenopausal women with osteoporosis compared raloxifene, alendronate and both therapies combined. Combination therapy resulted in greater BMD gains than either medication alone.48 There is no clear role for these combinations at present.
Limited studies combining MHT (including raloxifene) with teriparatide show greater BMD gains.49 No trials have combined MHT with denosumab.
Given its efficacy, why is MHT so controversial?
Two decades ago, oestrogen-alone and combined oestrogen–progestogen were widely used by postmenopausal women. In addition to reducing vasomotor symptoms, observational studies (e.g. Nurses’ Health Study) suggested that MHT was beneficial for cardiovascular health.50 Other studies (e.g. Framingham Study) did not support these findings.51 The WHI study was established specifically to assess the effect of MHT on cardiovascular health, with recruitment deliberately skewed towards older women (almost 70% of participants were aged 60 years or older).
The WHI compared placebo with oestrogen-alone (CEE) in 10,739 women who had had hysterectomies and compared placebo with combined oestrogen–progestogen treatment (CEE and medroxyprogesterone acetate) in 16,608 women who had not had hysterectomies.52 Secondary outcomes included breast cancer, colon cancer, stroke, thromboembolism and fracture risk. Both WHI arms were terminated early – the combined therapy arm in 2002, after 5.2 years, and the oestrogen- alone arm in 2004, after 6.6 years. The termination of the oestrogen–progestogen arm was announced by a publication with a contemporaneous press release – without prior knowledge of the principal investigators, and before final analyses had been done.53 Subsequent (and final) analyses of the WHI study have not necessarily agreed with the initial publications, particularly their tone.
Around the same time, results of the Million Women Study, an observational study of 1,084,110 women with longitudinal follow-up, were also published. This study concluded that invasive breast cancer was increased in women currently using MHT, particularly those using combined MHT, compared with those who had never used it.54
Consequently, MHT prescribing declined drastically worldwide, including in Australia.55 Some studies have since suggested a decrease in breast cancer incidence in women over the age of 50 years, attributed to the decreased use of MHT. For example, a 6.7% decrease in the incidence of breast cancer in Australia was reported in the year after publication of the WHI trial,56 although this would be inconsistent with the usual timeframe between cancer initiation and clinical presentation. Other changes during this time included increased intensity of breast cancer screening regimens in multiple countries (including the United Kingdom and Australia), increased rates of obesity and reduced rates of smoking. Notably, in 2007, there was a 34% increase in breast cancer compared with expected rates projected from 1987, despite widespread abandonment of MHT.57
More recently, there has been increasing recognition that the risks and benefits of MHT are more nuanced than were initially presented and that, for many women, MHT may be both beneficial and low risk.53
WHI and cancer risk
Breast cancer
Initial publications and press releases from the WHI study strongly implied that MHT increased the risk of breast cancer. The data showed that oestrogen-alone did not increase breast cancer, with an absolute risk in the oestrogen-alone arm of seven fewer cases of invasive breast cancer per 10,000 person-years of treatment compared with placebo.17 Combined oestrogen–progestogen slightly increased the risk of invasive breast cancer and all breast cancer, with an absolute risk of nine breast cancer cases per 10,000 person-years of treatment (i.e. less than 0.1% per person-year) (Table 2).18,58 This risk is similar to that seen with postmenopausal obesity and decreased physical activity.59,60 Importantly, extended follow up (18 years, including the intervention phase) has found no difference in mortality from breast cancer in the pooled intervention arms compared with placebo.61
{kind=link}
Endometrial cancer
Women in the oestrogen-alone arm of the WHI study had all undergone hysterectomy.17 There was no difference in endometrial cancer with combined oestrogen–progestogen compared with placebo (Table 2).18
Colorectal cancer
Combined oestrogen–progestogen reduced colorectal cancer compared with placebo.18 No difference was observed with oestrogen- alone compared with placebo (Table 2).17
WHI and cardiovascular disease
Coronary heart disease
This was the primary outcome measure of WHI. Early reports of the WHI study described an increased incidence of coronary heart disease (CHD) with combined oestrogen–progestogen compared with placebo, but not with oestrogen-alone (Table 2).18 Post hoc analyses suggested a critical 10-year window after menopause: in women aged 50 to 59 years, there was no increase in CHD in either arm and indeed a nonsignificant trend toward cardioprotection, particularly with oestrogen-alone, translating to 11 fewer cases of CHD per 10,000 patient-years.58 In contrast, an analysis combining the results of both treatment arms of the WHI study showed that MHT initiated more than 10 years after menopause conveyed no cardiac benefit, with a trend to increased risk.62
These conclusions are supported by the Early versus Late Intervention Trial with Estradiol (ELITE), which found that, compared with placebo, oestrogen (plus vaginal progesterone in women with a uterus) reduced the rate of increase of carotid artery intima–media thickness in women in whom MHT was initiated within six years of menopause, but not in those in whom it was initiated more than 10 years after menopause.63 A Cochrane review also found decreased CHD and lower mortality in women who commenced MHT within 10 years of menopause.64
Concerningly, stopping MHT may have adverse cardiovascular consequences. Several studies, including the Women’s International Study of Long-Duration Oestrogen after Menopause (WISDOM), were stopped prematurely because of the WHI publications. A Finnish study found that there was an increased risk of cardiac death in women aged under 60 years in the year after MHT discontinuation (standardised mortality ratio [SMR], 1.52; 95% CI, 1.13–2.00 after less than or equal to five years’ exposure; SMR, 2.08; 95% CI, 1.44–2.90 after more than five years’ exposure).65
Pulmonary thromboembolism and deep venous thrombosis
Pulmonary thromboembolism (PTE) and deep venous thrombosis (DVT) are increased with some forms of MHT. In the WHI study, DVT and PTE were increased with combined oestrogen–progestogen, with an absolute risk of eight additional PTEs per 10,000 patient-years and with the greatest risk in the first two years of use.18 With oestrogen-alone, only the increase in DVT reached statistical significance; the increase in PTE risk was not significant (Table 2).17
Stroke
Stroke was increased in both treatment arms of the WHI study, compared with placebo, amounting to an absolute risk of 12 additional strokes per 10,000 person-years in the oestrogen-alone arm and eight in the combined treatment arm (Table 2). Stroke risk was not affected by time since menopause at time of MHT initiation. Extended follow up has not shown any increase in stroke mortality.61
Does the type of oestrogen or oestrogen–progestogen matter for CHD risk?
Oral oestrogens increase clotting factors and inflammatory markers, an effect not seen with transdermal oestrogen, which bypasses first-pass hepatic metabolism.66,67 Observational studies have suggested reduced risks of cardiovascular disease (CVD), stroke and PTE with transdermal compared with oral oestrogen preparations.68-71 However, this has not been assessed in head-to-head studies.
The promiscuity of progestogen binding to multiple receptor types, with differing affinity and action (agonist vs antagonist effects), can result in quite different risk profiles for different progestogens, which may include CVD risk. However, this is conjectural, and the contribution of progesterone to thrombogenesis is unknown.
Side effects of SERMs, TSECs and tibolone
Both raloxifene and lasofoxifene reduce the risk of breast cancer.25,27 Preclinical evidence suggests bazedoxifene may also reduce the risk of breast cancer.72,73 Tibolone should not be used in women with a history of breast cancer due to an increased risk of recurrence.74
SERMs increase the risk of thromboembolism (both DVT and PTE).25,27,75 An increased risk of thromboembolic disease has not been reported with tibolone.29
Raloxifene increases the risk of fatal but not overall stroke (HR, 1.49; absolute risk of seven more cases per 10,000 women).76 In contrast, lasofoxifene reduces the risk of stroke.27 Tibolone is associated with increased stroke risk in older women.29
Overall, raloxifene does not reduce coronary artery disease,25,77 although the Raloxifene Use for The Heart (RUTH) study (in women with established CHD or risk factors for CHD) suggested a protective effect in women aged under 60 years (p for interaction of age with coronary artery disease, 0.01).77 Lasofoxifene reduces CHD at higher (0.5 mg) but not lower (0.25 mg) daily doses.27
SERMs may worsen vasomotor symptoms, whereas TSECs may reduce them. Tibolone is less effective than oestrogen or oestrogen–progestogen for vasomotor symptoms.74
Clinical indications for MHT use for bone health
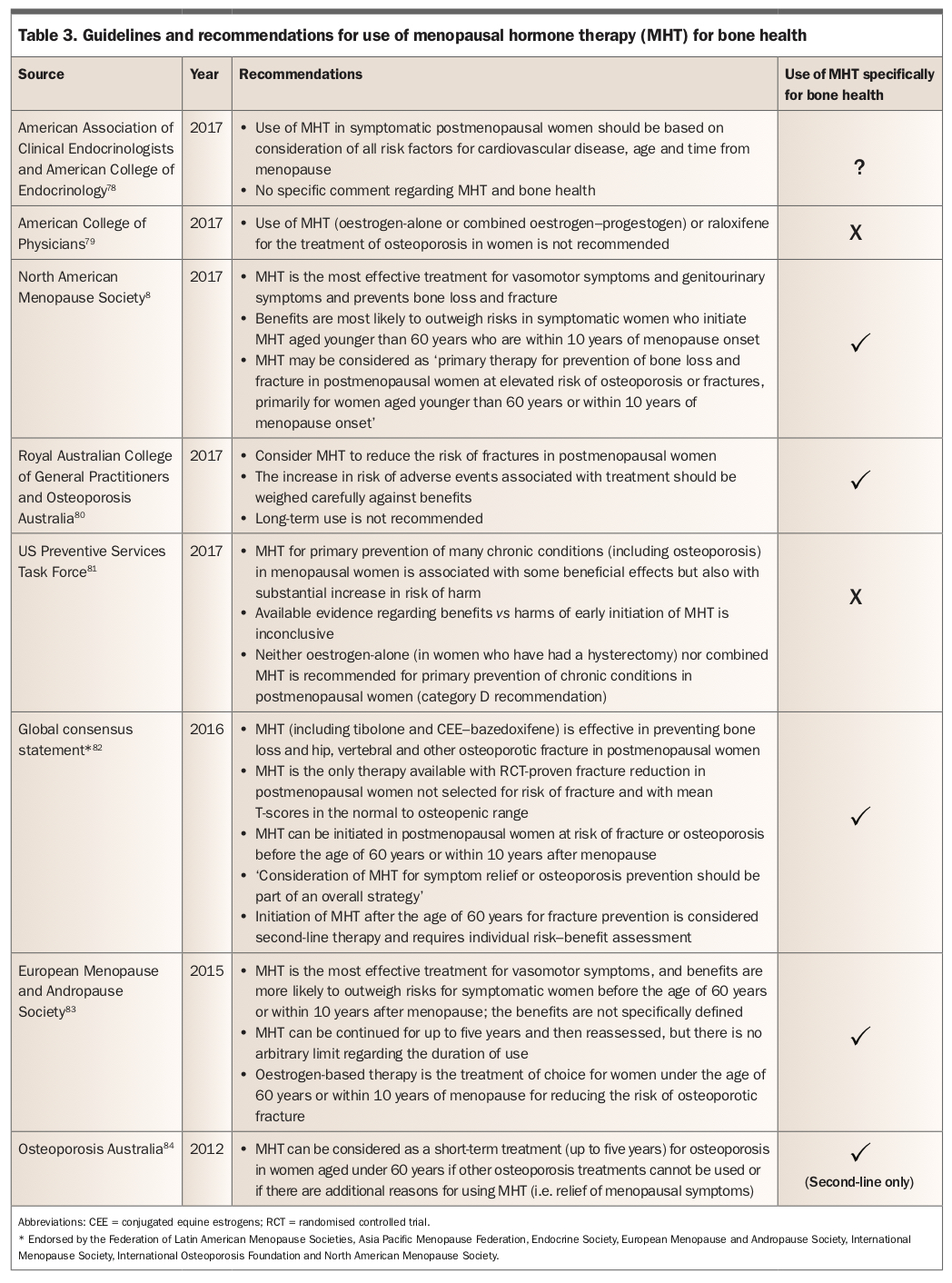
There are many guidelines regarding use of MHT (Table 3).8,78-84 Generally, there is concordance that MHT is appropriate and effective for vasomotor symptoms, assuming no contraindications.85 There is much less consensus regarding the use of MHT primarily for prevention or treatment of osteoporosis, particularly as a first-line agent, and questions regarding age of initiation, duration and monitoring of MHT are largely unanswered.
{kind=link}
Recommendations for MHT use
The Global Consensus Statement on Menopausal Hormone Therapy, ratified by multiple professional societies (Federation of Latin American Menopause Societies, Asia Pacific Menopause Federation, Endocrine Society, European Menopause and Andropause Society, International Menopause Society, International Osteoporosis Foundation and North American Menopause Society), states that MHT can be considered as second-line therapy for prevention of fractures in women who do not meet specific exclusion criteria (e.g. if antiresorptive agents are contraindicated or not tolerated). However, MHT is not recommended as first-line therapy.82
Additionally, many societies have published their own guidelines supporting use of MHT (Table 3). Most suggest that women under the age of 60 years or within 10 years of menopause may have a risk–benefit analysis favouring treatment. In general, these young women are at low risk of cardiovascular or cerebrovascular events, and their absolute risk of breast cancer is low.
{kind=link}
Guidelines supporting MHT use for bone health do not necessarily address questions such as optimal monitoring during treatment, when to stop, and how to ameliorate subsequent fracture risk after stopping.
Recommendations against MHT use
The US Preventive Services Task Force (USPSTF) and the American College of Physicians (ACP) advise against use of MHT solely for bone health.
The USPSTF acknowledged the clear fracture benefits of MHT in the WHI study but recommended against using MHT for primary prevention of osteoporosis, given its other risks. Whether ‘primary prevention’ encompasses women with osteopenia or osteoporosis by BMD criteria alone and/or prior fracture is unclear.81
The ACP concluded that MHT has no evidence of fracture benefit in women with established osteoporosis. Notably, the ACP specifically excluded WHI data from its assessment because WHI participants were not selected based on baseline bone health.79
Monitoring during MHT use for osteoporosis
There are no specific monitoring requirements for MHT used for bone health (e.g. BMD follow up), as opposed to general comments regarding MHT use for treatment of menopausal symptoms. Local guidelines should be consulted.
MHT contraindications and adverse side effects
The North American Menopause Society 2017 position statement recommends the following as contraindications to MHT: unexplained vaginal bleeding, active liver disease, prior oestrogen-sensitive breast and endometrial cancer, CHD, stroke, dementia, history or inherited risk of venous thromboembolism, porphyria cutanea tarda and hypertriglyceridaemia. Adverse effects that should be discussed with women considering MHT are nausea, bloating, weight gain, fluid retention, mood swings, breakthrough bleeding, worsening migraines, leiomyoma growth and exacerbation of endometriosis.8
Cessation of MHT
After cessation of MHT, cardiovascular risk will increase; this is often forgotten. Rapid bone loss will also ensue after cessation, as is observed after natural menopause. Alternative osteoporosis-specific treatment should be offered to women at high risk of fracture.
Conclusion
Use of MHT is justified in its own right for treating distressing vasomotor symptoms; this is discussed in the societal guidelines listed in Table 3.
MHT improves BMD and reduces fracture risk in women across the BMD spectrum, as seen in the WHI trial. However, the absolute benefit of treatment will be greater in women at higher risk of fracture (e.g. BMD T-score less than –2.5 or previous fracture). The use of MHT for the sole indication of primary prevention of osteoporosis in all postmenopausal women, irrespective of BMD, seems excessive. However, shutting the stable door before the proverbial horse has bolted is a concern for many women.
MHT is a valid option for younger postmenopausal women (within 10 years of cessation of menses) who have osteopenia or osteoporosis by BMD criteria, or previous minimal trauma fracture, and without specific contraindications. However, it should be noted that women with previous fracture are eligible for other agents to treat osteoporosis (albeit with their own long-term side effects) and that absolute fracture risk at this young age, even in women with low BMD, is low.
Notwithstanding the above, the influence of the WHI study is such that many women are fearful of MHT and many doctors are reluctant to prescribe it. Ongoing education of the wider medical community regarding the true findings from the WHI study remains important. As with any medication, prescribing MHT requires an informed discussion about risks versus benefits. These vary from woman to woman and include age, time since menopause, other risk factors for fracture (e.g. previous fracture) and other risk factors for CVD (e.g. smoking).
The choice of MHT preparation should be tailored to the individual patient’s clinical profile and preference. Transdermal therapies may confer a lower risk of CVD than oral preparations.
Optimal duration of MHT is unclear. Whether the adverse consequences of treatment observed in women initiating MHT at an older age apply to women who start MHT in the immediate postmenopausal period and continue use to this same age is unknown. As a rule of thumb, many endocrinologists would consider initiating, and continuing, MHT until the age of 60 years. The decision to cease MHT is an individual one, and many women may choose to continue treatment beyond this age for various reasons, including improved quality of life. After cessation of MHT, management of cardiovascular risk and fracture risk will need re-evaluation. ET