Diabetic foot ulcers: is remission a realistic goal?

Jump To
Diabetes complications
Diabetic foot ulcers are an underappreciated leading cause of the global burden of disease. A key to reducing this burden is not only healing them, but also preventing their recurrence and prolonging remission.
- Diabetic foot ulcers are common, complex and costly and a leading cause of Australia’s morbidity and mortality burdens.
- Reasons for this include the large number of people affected, sinister risk factors causing the ulcers, the complex management required to heal ulcers and high recurrence rates.
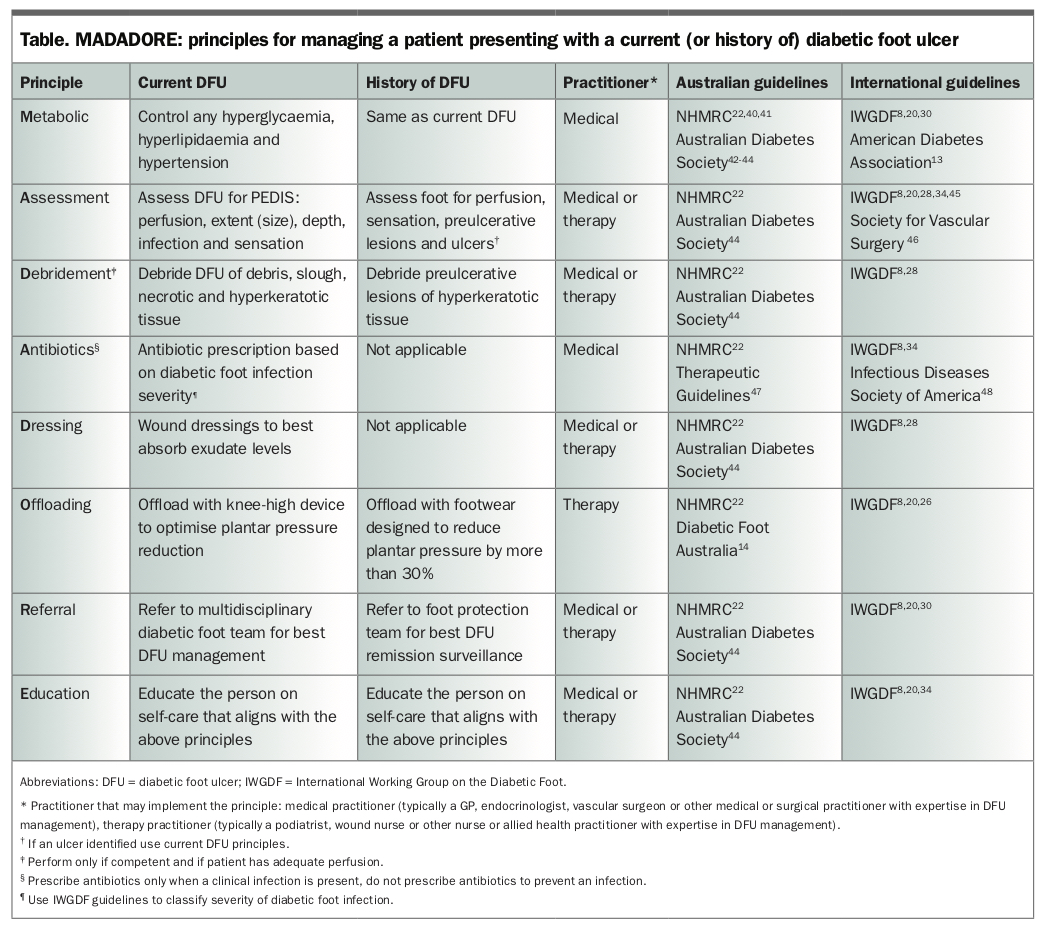
- Best-practice healing management and prevention of recurrence necessitates a multidisciplinary approach that considers: metabolic control, assessments of feet, debridement, antibiotics, dressings, offloading pressure, referral to multidisciplinary teams and education (MADADORE).
- Care planning that systematically employs these multidisciplinary management principles minimises time taken for diabetic foot ulcers to heal and maximises time in remission.
Diabetic foot ulcers (DFU) have been described as Australia’s least known major health problem as they receive little attention despite their significant contribution to the national prevalence, morbidity and mortality burdens.1-5 At any one time, an estimated 50,000 Australians have a DFU and at least another 50,000 have a history of DFUs.1,5 DFUs are reported to be Australia’s leading cause of amputation, a top-10 cause of disability, a top-20 cause of hospitalisation and to have five-year mortality rates that are worse than those for many cancers.1-5
Global and Australian research has consistently shown that best-practice multidisciplinary DFU management can prevent up to 85% of these burdens.1,6-9 Most research in this field has targeted healing DFUs.8,10,11 However, with 40% annual recurrence rates after healing, preventing recurrence and prolonging remission offers the greatest potential for progress in reducing this common, complex and costly global burden.12
Healing DFUs typically involves multidisciplinary diabetic foot teams in tertiary care, whereas prolonging remission involves GPs, podiatrists and other health practitioners in primary and secondary care. Fortunately, high-quality research has begun to focus on interventions that prevent DFU recurrence and prolong remission.10,12 This article reviews the factors that cause DFUs and the best-practice management required to heal them, and then focuses on interventions that could potentially make DFU remission a realistic goal.
What causes diabetic foot ulcers?
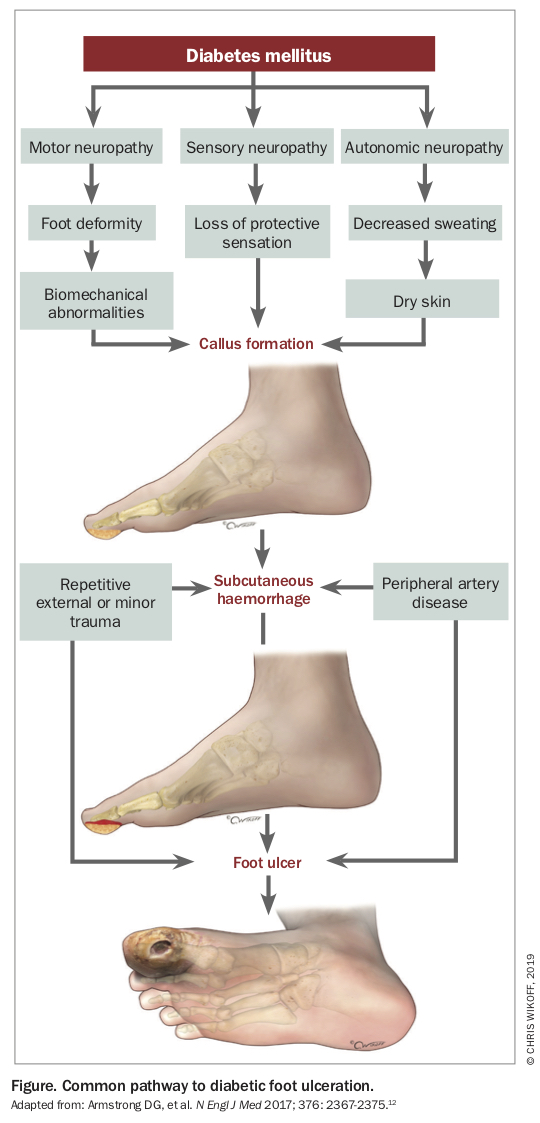
The most common pathway from diabetes diagnosis to DFU development is shown in the Figure.12 Diabetic peripheral neuropathy is the most crucial factor in this pathway.1,12 Patients with DFUs rarely present without precipitating neuropathy.1,12 Neuropathy typically develops five to 10 years after the onset of diabetes as the result of prolonged periods of hyperglycaemia, hyperlipidaemia and hypertension.8,12,13 Further, neuropathy rarely comes with warning signs such as pain or discomfort, but is rather a more sinister complication that causes the person to lose the ‘gift of pain’ to detect trauma to their feet.8,12 Thus, DFUs most commonly develop after some form of trauma to the feet of a person with neuropathy who cannot detect this trauma.8,12 The trauma typically results in a break of the skin and can be acute or chronic in nature.8,12 Acute trauma may include a puncture wound from standing on a foreign object, an ingrown nail from poor self-care or burns from standing barefoot on a hot path.8 Chronic trauma may include fungal infections from wet macerated skin between the toes, friction from incorrectly fitting shoes or dry heel fissures resulting from autonomic neuropathy.8
{kind=link}
The most common trauma resulting in DFU is from the chronic repetitive mechanical pressure experienced underneath the feet from walking (plantar pressure).12,14 When plantar pressure becomes too high in people without neuropathy, they experience pain or discomfort and subconsciously adjust their gait to try to offload these areas of higher plantar pressure.12,14 However, without pain, people with neuropathy have no warning signs and do not adjust their gait.12-14
As neuropathy worsens it can cause changes in gait and foot deformities, which can further elevate high plantar pressures.15-17 Such changes may include postural instability; reduced flexion of the ankle, knee and hip; intrinsic foot muscle wasting; contraction of the Achilles tendon; clawing of the toes; longer stance time and shorter step length.15-19 Additionally, any minor amputation procedure (i.e. below the ankle) is also highly likely to further elevate high plantar pressure areas due to the reduction in the plantar surface area and further gait changes to adjust for the loss of function after amputation.12-14
Repetitive high plantar pressures result in calluses, corns or blisters. In a person with neuropathy these are known as preulcerative lesions. Without treatment, preulcerative lesions cause subcutaneous haemorrhage in the plantar tissue that eventually develops into a DFU.8,12,20 All patients with DFUs, and especially those with concomitant peripheral artery disease (PAD), need best-practice treatment to heal.8,12 If not treated properly, infection is highly likely. Infection significantly increases the risk of hospitalisation and amputation.8,12
How do we best manage diabetic foot ulcers?
Over the past 30 years, expert multidisciplinary diabetic foot teams have been shown to be more effective in managing DFUs compared with solo expert health practitioners.8,12,21-23 The reasons for this are highlighted by the International Working Group on the Diabetic Foot (IWGDF):24
- Prevention of foot ulcers in at-risk patients with diabetes (i.e. those with neuropathy)20,25
- Footwear and offloading interventions to prevent and heal DFUs26,27
- Interventions to enhance the healing of DFUs28,29
- Management of PAD in patients with DFUs30-33
- Management of infection in patients with DFUs.34,35
To effectively heal a DFU, and prevent recurrence, expertise is required in the management of risk factors, pressure offloading, wound dressing interventions, PAD and infection.20,26,28,30,34 In addition, the 77 IWGDF guideline recommendations indicate that expertise is also required in metabolic control, debridement, chronic wound healing, revascularisation, other surgical procedures and patient education.20,26-28,30 The NHMRC Australian diabetic foot guidelines (although now more than eight years old) also strongly recommend referring patients to multidisciplinary diabetic foot teams for effective management of DFUs.22
How do GPs best manage diabetic foot ulcers?
People with DFUs rarely present to a multidisciplinary diabetic foot team without first seeing their GP or another health practitioner for assessment, management and referral.36-39 To assist GPs to quickly remember the guideline-recommended DFU principles needed to manage a patient presenting with a DFU for the first time, we have devised the acronym ‘MADADORE’ (Table).
It is strongly recommended that the GP urgently organises to share the care of the patient with their local multidisciplinary diabetic foot team (if available) after this first presentation. The evidence shows that the earlier a GP refers a patient to a multidisciplinary diabetic foot team (less than two days) the more likely the ulcer will heal quickly and the less likely the patient will develop infection, be hospitalised or require an amputation.36-39,49 Patients should be assessed by such a team on a weekly or biweekly basis with regular multidisciplinary care plans and communications shared with the patient and their GP for mid-week dressings and other medical management until healed.44 The multidisciplinary diabetic foot team should comprise health practitioners who have the competencies or experience to perform all the evidence-based principles (MADADORE; Table).20,22,26,28,30,34,50 At a minimum, this should include a medical practitioner (typically an endocrinologist or vascular surgeon) and therapy practitioner (typically a podiatrist or wound nurse) who work together for at least one session a week solely managing DFUs according to best practice principles.8,22,23,44,50 The team should also have direct access to other medical, surgical, nursing and allied health practitioners when complexity dictates; for example, a vascular surgeon when the patient also has PAD, or an infectious diseases consultant when the patient has moderate-to-severe infection such as spreading cellulitis or osteomyelitis.8,22,23,30,34,44,50
{kind=link}
The evidence-based management principle arguably implemented most poorly – but with the highest quality evidence for healing a DFU – is the provision of optimal offloading of the elevated high plantar pressure areas that typically precede and are often the cause of a DFU.8,22,26,27,44,51-53 The gold standard offloading intervention is a removable or nonremovable knee-high offloading device such as a total contact cast or prefabricated walker or moonboot.8,26 Evidence suggests that DFUs in about two-thirds of patients engaging with these best-practice multidisciplinary team management arrangements will heal within three months.36,38,54 However, if access to a multidisciplinary diabetic foot team is limited locally, then Australian guidelines recommend patients are managed by a GP working together with a podiatrist or wound nurse, with telehealth services used to access expert advice from a larger multidisciplinary diabetic foot team using digital images.22,44 This is an ongoing area of research and implementation.
How do we best prolong diabetic foot ulcer remission?
Once healed, regular surveillance and action by health practitioners with DFU expertise remains of utmost importance. A healed DFU is highly susceptible to recurrence, but also responds well to best-practice interventions.10,12 A recent high-quality review of DFU recurrence found recurrence rates of 40% at one year, 60% at three years and 75% at 10 years.10,12 However, it also found that several interventions reduced these recurrence rates by 31 to 62%.12 We review these remission-prolonging interventions below.
The interventions identified as most effective in reducing recurrence were integrated foot care, therapeutic footwear, certain prophylactic surgical procedures and patient self-management strategies.10,12,14,20,25-27 Furthermore, these meta-analyses found the interventions were even more effective when patients were engaged and adherent with them.10,12
First, integrated foot care is typically defined as one to three-monthly surveillance by a podiatrist (or equivalent therapy health practitioner) to identify and manage preulcerative lesions.12,20,22 Preulcerative lesions are calluses, corns or blisters that form in response to chronic high plantar pressure areas in a person with neuropathy.12,20 These are managed by reducing the high plantar pressure via debridement of the hyperkeratotic tissue and offloading strategies.12,14,20,25,26 The most effective offloading strategies for preventing recurrence are therapeutic footwear and some prophylactic surgical procedures, which are further discussed below.12,14,26
Second, therapeutic footwear is arguably the most effective of all interventions to prevent recurrence.12,14,26 Therapeutic footwear is defined as any footwear designed to allow some form of treatment (e.g. an insole/orthoses or rocker-bottom profile) and can include custom-made or prefabricated medical-grade footwear (e.g. extra-deep or extra-wide footwear).14 Several high-quality randomised controlled trials have demonstrated that therapeutic footwear, when specifically designed to reduce high plantar pressure areas by more than 30%, are successful at prolonging remission.12,14,26 This means that the health practitioners prescribing and/or designing the footwear (typically podiatrists, orthotists or pedorthists) need to use validated plantar pressure equipment to measure the patient’s plantar pressures before the footwear is designed or modified.12,14,26 They need to design or modify the footwear and insoles with guideline-recommended features shown to reduce high plantar pressures by more than 30%, or continue the design process until this is achieved.12,14,26 These recommended features are dependent on the site of the previous DFU, but may include increasing or decreasing the top cushioning cover of an insole or orthosis, adding or repositioning a metatarsal pad or medial arch support, or adding or repositioning a rocker profile to the outsole.14,26 It is recommended that health practitioners consult the Australian guideline on footwear for people with diabetes to help with tailoring specific data-driven footwear recommendations and features for their patient.14
Third, if therapeutic footwear does not work, international guidelines recommend prophylactic surgical procedures that reduce high plantar pressures, including digital tendon flexor tenotomies, Achilles tendon lengthening, osteotomies, joint arthroplasties and metatarsal head resections.12,26 Digital flexor tenotomies and Achilles tendon lengthening in particular have demonstrated great potential in preventing DFU recurrence and are currently under investigation in large-scale robust randomised controlled trials.12,26,55
Finally, although patient education alone has not been shown to have any effect in reducing DFU recurrence, it has been shown to have large effect sizes when patients have put into practice self-management strategies, thus highlighting the impact of adherence and self-management.12,20 Effective patient self-management strategies include adhering to regularly inspecting the feet for preulcerative lesions, measuring temperatures of the feet to detect inflammation, wearing prescribed therapeutic footwear inside and outside the home, attending integrated foot care surveillance and review of their offloading strategies, and urgently acting on any suspicious foot changes.10,12,20 These self-management strategies arguably show the most promise in prolonging future remission.10,12,20 Furthermore, preliminary studies on innovative self-monitoring devices such as infrared thermal imaging, smartphone apps, plantar pressure-measuring insoles and other wearables technologies are also showing much promise.12,12,27,56-59 It is envisaged that such technological advancements will further engage patients and their health practitioners in strategies that identify and prevent preulcerative lesions much earlier and, in turn, significantly prolong remission.
How do GPs best prolong diabetic foot ulcer remission?
The same overarching principles outlined for patients with current DFUs are the best interventions to prevent recurrence in a patient presenting with a DFU history but with an emphasis on prevention of recurrence. The evidence suggests prolonging DFU remission requires implementing similar best practice management principles as for healing, including metabolic control, assessment, debridement, offloading, referral and education. Instead of focussing on the ulcer, the focus is on preulcerative lesions and especially the sites of previous DFUs.
Conclusion
DFU remission is a realistic goal but is typically only achieved in patients with health practitioners who are aware of the seriousness of the condition and the best-practice multidisciplinary principles to manage it, and who systematically employ these principles when managing their patients. Making remission a more realistic goal for all patients with a DFU requires broader awareness of the seriousness of this condition, incentives to promote best-practice multidisciplinary and self-management interventions, and investment in research and development that targets earlier surveillance, identification and self-management in patients with a history of DFUs. ET