Hypothyroidism: how to make the diagnosis and when to treat it
Thyroid diseases
Endocrine diseases
Hypothyroidism may be obvious clinically but it has a wide spectrum of severity and can be very subtle. Many people with normal thyroid function may present to their GP with mild symptoms that suggest hypothyroidism; therefore, biochemical confirmation of true hypothyroidism is mandatory. There is no evidence that levothyroxine treatment of suggestive symptoms is beneficial when the thyroid stimulating hormone level is normal.
- Hypothyroidism is a common condition, with most people having subclinical hypothyroidism.
- The most common cause of hypothyroidism in Australia is autoimmune thyroid disease.
- A clinical diagnosis of hypothyroidism should be considered in the presence of one or more of its classic symptoms and signs.
- People with normal thyroid function may complain of mild symptoms that suggest the possibility of hypothyroidism; therefore, biochemical confirmation is mandatory.
- Synthetic levothyroxine is the best standard replacement therapy for patients with hypothyroidism.
Hypothyroidism is a common condition. When the whole spectrum of disease is considered it affects 4.6% of the population (4.3% with subclinical hypothyroidism and 0.3% with overt disease).1 Over 11% of the population are positive for thyroid peroxidase antibodies.1 Severe hypothyroidism (myxoedema), although usually easy to recognise clinically, is uncommon. Most cases of hypothyroidism are diagnosed on suspicion based on one or more milder symptoms and signs that are not pathognomonic, or the finding of a raised thyroid stimulating hormone (TSH) level in asymptomatic individuals as part of healthcare screening. Autoimmune thyroid disease is the most common cause of thyroid dysfunction in our community and accounts for the higher prevalence of thyroid dysfunction in women.
Causes
Deficiency of thyroid hormone is usually due to damage to the thyroid gland itself (primary hypothyroidism), but can also result from impairment of pituitary function with diminished TSH drive to the thyroid gland. In this circumstance, either the pituitary gland itself is damaged (secondary hypothyroidism) or there is a loss of hypothalamic signal to the pituitary (thyrotropin-releasing hormone [TRH]) due to hypothalamic disease (tertiary hypothyroidism). As secondary and tertiary hypothyroidism are often difficult to distinguish, they may together be termed central hypothyroidism. The different causes of hypothyroidism are listed in the Box.
{kind=link}
Making the diagnosis
Clinical diagnosis
Hypothyroidism should be considered in the presence of one or more of its classic symptoms and signs, including chronic tiredness, poor mental concentration, depression, weight gain, constipation, myalgia, dry skin and hair, facial puffiness, general weight gain and husky low-pitched voice. Hypothyroidism should be excluded in people with psychosis and in those with apparent dementia or an unexplained neurological disorder. Hypothyroidism may be obvious clinically but has a wide spectrum of severity and can be very subtle. Conversely, many persons with normal thyroid function complain of mild symptoms that suggest the possibility of hypothyroidism (Figure); therefore, biochemical confirmation is mandatory.2 There is no evidence for benefit from levothyroxine treatment of suggestive symptoms when the TSH level is normal nor is there a role for levothyroxine use in euthyroid individuals who have obesity, depression or urticaria.3
{kind=link}
Biochemical diagnosis
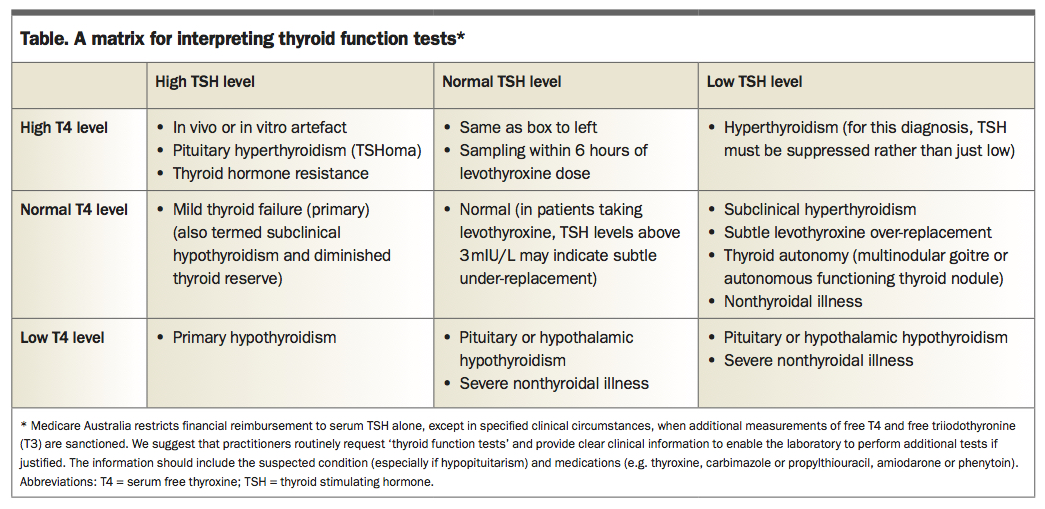
Primary hypothyroidism is characterised by a raised serum TSH level with a low free thyroxine (T4) level. Subclinical hypothyroidism (also known as mild thyroid failure) is defined by a raised TSH level but free T4 level within the normal range (Table).4 These definitions raise the question of the true reference ranges particularly for TSH. The upper limit of the normal range of TSH is usually described as 4 to 5 mIU/L but a lower limit of about 3 mIU/L has been advocated. However, without evidence of benefit of treatment for borderline TSH, an upper limit of about 4 to 5 mIU/L is still generally recommended.5 Indeed, in the very elderly (over 85 years of age) the normal range of TSH may be extended up to about 7 mIU/L and one epidemiological study has even suggested a survival benefit for higher TSH levels.6
{kind=link}
Secondary hypothyroidism is characterised by a low free T4 level with the TSH level within the reference range. Milder forms should be suspected in the appropriate clinical context if the free T4 level is low-normal.
In the individual person, the free T4 range is more tightly regulated than the population normal range.7 A low-normal value may thus occasionally raise concern about hypothyroidism but, when the TSH level is normal, this should not be interpreted as primary hypothyroidism, and only as secondary hypothyroidism if there is other evidence to support hypothalamo-pituitary disease.
Autoimmune thyroid disease is the most common cause of primary hypothyroidism. Measurement of thyroid peroxidase antibodies (aTPO) is the most sensitive test for thyroid autoimmunity and renders measurement of antithyroglobulin antibodies (aTg) redundant. In overt primary hypothyroidism, identification of thyroid autoimmunity does not influence the levothyroxine treatment decision but has an explanatory value for the patient and indicates a risk of other autoimmune disease (e.g. atrophic gastritis and pernicious anaemia) that is relevant to follow up. With a raised TSH level alone, the presence of aTPO increases the risk of progression to overt hypothyroidism.
There is no routine role for thyroid imaging in the diagnosis or management of hypothyroidism. Imaging should only be performed for specific reasons (e.g. in the assessment of a specific nodule). Hashimoto’s thyroiditis is typically nodular when advanced and a thyroid nodule biopsy, when the diagnosis has been made serologically, is usually not necessary. A clinically apparent and enlarging nodule despite thyroid hormone treatment requires cytological examination by fine needle biopsy, particularly to identify if thyroid lymphoma may have developed. Thyroid lymphoma is a rare disease almost entirely confined to people with pre-existing autoimmune thyroid disease. Whether there is any increase in other thyroid malignancy in the presence of thyroid autoimmune disease remains unclear. The general guidelines for investigation of a thyroid nodule should be followed.8
Types of hypothyroidism
Severe hypothyroidism/myxoedema coma
The clinical manifestation of severe hypothyroidism is termed myxoedema, as described in the late 19th century, because of the marked generalised puffiness of nonpitting oedema. Muscle ache is common and because creatine kinase clearance is reduced with elevated creatine kinase levels, an incorrect diagnosis of myositis may be made.9 Intestinal pseudo-obstruction can occur. In general, especially if cardiac disease is present, initiation of levothyroxine at a very low dose, 12.5 to 25 mcg daily, and gradual increment of dose every few weeks may be necessary to avoid precipitating symptomatic cardiac ischaemia.
Severe hypothyroidism can be precipitated into myxoedema coma by intercurrent illness or cold exposure. In myxoedema coma, there is obtundation, hypoventilation, hypothermia, hypotension and hyponatraemia.10 If this condition is suspected, immediate transfer of the patient to a major hospital is appropriate.
Pregnancy-associated hypothyroidism
In women with established hypothyroidism it is important to optimise replacement levothyroxine dose preconception and to increase the dose in pregnancy to maintain optimal replacement. Fetal thyroid function does not develop before the 12th to 18th week of gestation, so before then the fetus requires maternal thyroxine, particularly for neurological development. Overt hypothyroidism, and possibly raised maternal TSH level alone, in pregnancy has been associated with a loss of IQ points in the offspring.11 Current guidelines advocate treatment with levothyroxine if the TSH level is above the normal assay-specific trimester-specific pregnancy range, which may be provided by the laboratory or, in the absence of this information, if the TSH level is above 4 mIU/L.8,12 If overt hypothyroidism is detected, then aggressive levothyroxine replacement at full dose should be immediately instituted to optimise fetal thyroxine supply and referral of the patient to an endocrinologist is recommended.
The change in immune state in pregnancy can cause induction of thyroid autoimmunity and either hypo- or hyperthyroidism. It is still debated whether assessment of thyroid function should be routine at diagnosis of pregnancy but certainly it should be performed if there is a high risk of thyroid disease.12
Transient hypothyroidism
Early in the course of Hashimoto’s thyroiditis, thyroid status can vary spontaneously and mild hypothyroidism can remit. After radioactive iodine (RAI) therapy for Graves’ hyperthyroidism, hypothyroidism occurring in the next six months can remit. Subacute thyroiditis typically has a transient hyperthyroid phase then a hypothyroid phase with subsequent re-establishment of the euthyroid state. In the absence of major symptoms, it is reasonable to continue monitoring without institution of replacement therapy until stable thyroid function, either hypothyroid or euthyroid, is apparent.
Post-radioiodine therapy hypothyroidism
Hypothyroidism can occur within a few weeks after RAI administration and may be biochemically severe. This can be transient and remit by six months after the dose.
Reduction of the dose and withdrawal of antithyroid drug therapy if continued after the RAI administration is the first step in management. If symptomatic, then levothyroxine therapy can be started, and the long-term need assessed by reduction and withdrawal at six to 12 months. This should be done in conjunction with the managing endocrinologist. There is a steady rate of development of permanent hypothyroidism after RAI for patients with Graves’ disease to about 50% by 10 years.13 Long-term yearly surveillance of serum TSH levels will detect this.
Subclinical hypothyroidism
A raised TSH level with a normal free T4 level has been termed subclinical hypothyroidism, although the occasional patient is in fact symptomatic. The free T4 value is usually toward the low end of the normal range, and symptoms are presumed to arise if the free T4 level is sufficiently lower than the individual free T4 set point. In the first instance it is important to establish that the abnormality is persistent over more than four to six weeks before diagnosing subclinical hypothyroidism, as transient TSH elevation is common.
A recent article reviewing published trials concluded that almost all adults with subclinical hypothyroidism (excluding women trying to conceive, those with a TSH level >20 mIU/L and young adults) would not benefit from treatment with thyroid hormones.14 Furthermore, a recent trial of levothyroxine therapy in adults over 65 years of age with subclinical hypothyroidism found there was no apparent clinical benefit over 12 months of use, nor evidence of harm.15 Although routine treatment of mild subclinical hypothyroidism with a TSH level below 10 mIU/L is not indicated, the data are insufficient to conclude this for people less than 65 years of age and symptomatic people, so that a treatment decision should be placed in the individual context of comorbidities, safety and patient preferences.16 Comorbidities such as dyslipidaemia and clinical assessment of likely progression (e.g. with concomitant presence of aTPO, which predicts progression to overt hypothyroidism at about 5% per year) are factors prompting treatment rather than monitoring alone.17 Risk of coronary disease associated with subclinical hypothyroidism does not differ by aTPO status.18 Most importantly, if the patient is intending to conceive or is already pregnant, treatment to normalise TSH level is indicated.12,19
Congenital hypothyroidism
One in 3500 live births is associated with congenital hypothyroidism usually due to athyreosis and occasionally to lingual thyroid (i.e. failure of normal fetal thyroid tissue migration). Failure to institute prompt levothyroxine replacement leads to permanent neurological deficit. For this reason, thyroid function assessment is a part of the universal newborn screening program by heel-prick blood testing with the aim of therapy by not later than the 10th postnatal day. Levothyroxine dosing needs to be carefully and progressively adjusted for age to prevent over- and undertreatment.20 Early treatment results in an excellent outcome.
Iodine-induced hypothyroidism
Iodine is an essential trace element for thyroid function. The recommended intake is about 150 mcg daily, and 200 to 250 mcg daily in women during pregnancy and when breastfeeding. This is less than a 5 g requirement over an average lifetime. Iodine is only stored within the thyroid gland and is a key component of thyroid hormone. Despite iodine being essential, excessive iodine intake can provoke thyroid dysfunction in the already diseased thyroid.21
The mechanisms of thyroid hormone synthesis may be chronically inhibited by excessive iodine, and quiescent autoimmunity may be activated. An intake of iodine of more than the recommended daily dose should therefore be discouraged. Iodine supplementation is usually not required except in women during pregnancy and lactation or in people who have a restricted diet (e.g. vegan). In pregnancy, excessive iodine intake can promote fetal goitre. Strong iodine solutions (e.g. Lugol’s iodine) should therefore only be used by thyroid surgeons or endocrinologists in preparation for thyroidectomy for treatment of Graves’ disease. Similarly, use of kelp tablets should be discouraged.
Amiodarone-induced hypothyroidism
The antiarrhythmic drug amiodarone is 37.2% iodine and liberates about 9 mg of iodine daily per 200 mg tablet and can thus cause iodine-induced hypothyroidism. The organic metabolite desmethylamiodarone is also toxic to the thyroid. Amiodarone-induced hypothyroidism tends to occur in an already diseased thyroid so that predose thyroid function tests to detect subclinical hypothyroidism and the presence of thyroid autoantibodies is useful, with routine monitoring every six months thereafter.22 Levothyroxine replacement therapy is usually straightforward and amiodarone, which may be necessary to treat a life-threatening arrhythmia, can be continued. Amiodarone can also cause hyperthyroidism, which may be severe and refractory to treatment, requiring high-dose prednisolone therapy and possible thyroidectomy. Prompt referral for endocrinologist management is essential.
Other drugs inducing hypothyroidism
Lithium has long been known to cause goitre and hypothyroidism due to inhibition of thyroid synthesis and release. The prevalence varies in different reports but overall is high with overt hypothyroidism in 8 to 19% of lithium users and subclinical hypothyroidism in 23% of users.23 Recently, the immune system activating monoclonal antibodies (ipilimumab, a CTL4 inhibitor; nivolumab and pembrolizumab, PD-1 inhibitors), which are used in metastatic malignant melanoma and increasingly for other metastatic tumours, have been found to cause a range of autoimmune diseases, including hypothyroidism and other endocrine diseases. Alemtuzumab, a monoclonal antibody against CD52 used in the treatment of relapsing-remitting multiple sclerosis, more commonly causes Graves’ hyperthyroidism, but can cause hypothyroidism. Some tyrosine kinase inhibitors (e.g. lenvatinib used in the treatment of advanced thyroid cancer) accelerate levothyroxine clearance and dose increment is required.
Associated conditions
Other autoimmune conditions are associated with Hashimoto’s thyroiditis. In more than 14% of cases of Hashimoto’s thyroiditis there may be one or more associated conditions, including pernicious anaemia/atrophic gastritis (so-called thyrogastric cluster), Addison’s disease, coeliac disease, vitiligo and rheumatoid arthritis.24 Patients should be clinically assessed at diagnosis and yearly thereafter, with measurement of serum B12 levels and with serological and other laboratory assessment of any clinical manifestations.
Nonthyroidal illness
Measurement of serum thyroid hormone levels is not an infallible guide to thyroid status. It is clear that profound alterations in thyroid hormone economy can occur in diseases not directly affecting the thyroid gland itself, leading to changes in thyroid hormone levels and diagnostic uncertainty. Overt hypothyroidism or hyperthyroidism can, however, be confidently diagnosed. As a general rule it is best to repeat testing in four to six weeks when changes due to nonthyroidal illness will usually have resolved.25
Severe nonthyroidal illness, causing a decline in free T4 levels, is a diagnostic challenge within the hospital intensive care unit. TSH levels, however, are not elevated acutely, so that in the absence of head trauma and possible pituitary damage, hypothyroidism can be discounted.
Treatment
Levothyroxine
Synthetic levothyroxine (Oroxine, Eutroxsig [available in 50, 75, 100 and 200 mcg tablets] and Eltroxin [available in 25, 50, 75, 88, 100, 112, 125, 137, 150, 175 and 200 mcg tablets]) is the best standard replacement therapy for patients with hypothyroidism due to its efficacy in resolving the symptoms of hypothyroidism, long-term experience of its benefits, favourable side-effect profile, ease of administration, good intestinal absorption, long serum half-life and low cost.26 Eltroxin is not exactly equivalent to Oroxine so dose restabilisation is required if a change of agent is made. Eltroxin is not required to be routinely refrigerated but should be stored below 25ºC. Oroxine and Eutroxsig should be stored long term at 2 to 8ºC, but tablets may be stored short term at 8 to 25ºC for up to 14 days. Oroxine and Eutroxsig are listed on the PBS, but currently Eltroxin is not. All brands of levothyroxine tablets should be kept dry and protected from direct sunlight and extremes of temperature.27 Short-term transport (e.g. from pharmacy to home) can be at room temperature.
The dose of levothyroxine best relates to lean body mass (1.5 to 3.0 mcg/kg daily), but in routine clinical care the usual adult dose is 100 to 150 mcg daily. In otherwise healthy adults an initial dose of 50 to 100 mcg daily can be increased after not less than four to six weeks (three to five half-lives), as necessary, targeting a serum TSH level of 0.5 to 2 mIU/L. In people over 60 years of age, especially in the presence of ischaemic heart disease or increased risk of arrhythmia, the TSH target should be less than 5 mIU/L. This can be achieved by starting levothyroxine at 25 to 50 mcg daily, occasionally at 12.5 mcg daily, increasing by 25 mcg daily not less than every four weeks.28 An initially very high TSH level may take months to normalise so that, for up to six months, the achievement of a satisfactory free T4 level in the mid-normal range should be accepted over TSH normalisation. Symptoms alone lack sensitivity and specificity and therefore should not be used to judge adequacy of replacement in the absence of biochemical assessment.
During pregnancy and before conception, the TSH target is normalisation to the assay-specific trimester range or less than 4 mIU/L.12 The increased metabolism of T4 in pregnancy requires a prompt adjustment of levothyroxine dose by 30 to 50% once pregnancy is confirmed. A simple initial adjustment is a double dose for two separated days of the week, and further adjustment by monthly thyroid function testing during pregnancy. The pre-pregnancy dose can usually be resumed postpartum. It is usual for an endocrinologist to supervise adjustment of levothyroxine dose during pregnancy. Continued specialist follow up may be appropriate for several months postpartum to manage thyroid dysfunction, which occurs in about 30% of patients if aTPO is positive.
In central hypothyroidism, the TSH level cannot be used as target and a mid-to-high normal free T4 value, regardless of the TSH level, is the aim. Dose selection and adjustment frequency is the same. Consideration should be given to the adequacy of other pituitary hormonal axes, in particular adrenal function. Levothyroxine replacement can render borderline hypoadrenalism overt due to increased steroid hormone clearance.
Levothyroxine should be ingested on an empty stomach usually in the morning avoiding concomitant medications, especially calcium or iron supplements.27
Liothyronine
Use of liothyronine (Tertroxin) is usually confined to transient use (at 20 to 40 mcg daily) replacing levothyroxine before whole-body radioiodine scanning during follow up of people with thyroid cancer. Genuine intolerance or allergic reactions to synthetic levothyroxine are rare and unresponsiveness is rarer still, therefore, chronic use of liothyronine alone is very rarely necessary.
Liothyronine therapy is difficult to manage because triiodothyronine (T3) levels vary markedly throughout the day in relation to time of ingestion (liothyronine has a half-life of 24 hours) so that thrice daily therapy is required to achieve T3 levels consistently within the normal range, and T4 levels will be low and not indicative of thyroid status. TSH level is the best biochemical index to use, but it is unclear if the nonphysiological variation of T3 levels from high to low throughout the day is without risk.
Combined therapy
Combined use of levothyroxine and liothyronine has been examined in many small trials in people dissatisfied with levothyroxine replacement alone and, when adequate blinding has been conducted, no clear clinical benefit has been identified.26 Combination therapy should never be routine and if trialled clinically, a liothyronine dose of 10 to 20 mcg daily is generally used, with monitoring using TSH measurement to regulate the dose and avoid TSH suppression.
Thyroid extract, which contains both levothyroxine and liothyronine, is supplied by compounding pharmacists, and is often advocated by fringe practitioners. For 50 years, desiccated thyroid extract was the routine form used until synthetic levothyroxine, with a more precise dosage, became available. The relative T4 to T3 content of thyroid extract is difficult to standardise, leading to a risk of variable under- or over-dosage. Furthermore, an animal source product with potential for prion infectivity is generally to be discouraged if a pure synthetic form is available. Thyroid extract has never been submitted for assessment of efficacy or safety by regulatory agencies. Its use cannot therefore be recommended. Should it nevertheless be used, monitoring with measurement of TSH levels is essential.
Monitoring
In general, once the correct dose of levothyroxine has been achieved, the required dose remains stable and only yearly thyroid function test monitoring is routinely required. With decrease of lean body mass in advanced age, a decrease in dose may be required.
If symptoms persist despite optimisation of serum TSH level (0.5 to 2 mIU/L), evaluation for causes other than hypothyroidism should be undertaken. If the TSH level fails to normalise despite an apparently appropriate levothyroxine dose, adherence to therapy should be reviewed, drugs interfering with levothyroxine absorption should be excluded, and gastrointestinal diseases impairing levothyroxine absorption (e.g. coeliac disease, atrophic gastritis, Helicobacter pylori infection) should be considered. If adherence to daily treatment is poor and cannot be improved, weekly oral administration of the full week’s dose of levothyroxine should be considered.
Often there is no available documentation of hypothyroidism in a person taking levothyroxine therapy. If it is appropriate to re-establish the need for levothyroxine therapy then it can be ceased for five weeks and then if the TSH level is elevated, primary hypothyroidism is confirmed.29 A high dose can be reduced initially rather than ceased.
Role of the GP
GPs are in an excellent position to suspect, diagnose, treat and monitor patients with hypothyroidism. Although the development of hypothyroidism can be subtle and insidious, sometimes rendering the new medical observer at an advantage to the regularly seen doctor, a high index of suspicion for hypothyroidism with any related symptoms promotes sensitive case-finding. To assist in the management decisions in patients with primary hypothyroidism – overt or subclinical hypothyroidism – a Flowchart is provided.
Patients should be referred to an endocrinologist if test results are unusual or difficult to interpret, central hypothyroidism is suspected because of a lack of elevation in TSH level, or the response to treatment is inadequate. Education promotes optimal adherence to therapy. GPs should emphasise that levothyroxine is a life-long replacement therapy and not a curative treatment.
Conclusion
Mild hypothyroidism is common and usually due to autoimmune thyroid disease. The diagnosis is rarely obvious clinically and confirmatory biochemical testing should be performed for suggestive symptoms. A raised TSH level is indicative of primary thyroid failure. In general, if the TSH level is above 10 mIU/L there will be a clinical benefit from treatment. Synthetic levothyroxine is the treatment of choice, adjusted to optimise TSH into the normal range. Maintenance of a normal TSH level in pregnancy is of particular importance for fetal development and pregnancy outcome. In women already taking levothyroxine, an increase in dose of levothyroxine in pregnancy is required and specialist referral is usually appropriate. It is important to advise all patients on the need to maintain long-term stable therapy. Monitoring outside of pregnancy is generally only required annually. ET