Laufala is a 25-year-old primigravid woman of Samoan ethnicity who presents to your medical centre for her first antenatal visit, estimated at eight weeks’ gestation based on her last menstrual period. Her past medical history includes polycystic ovary syndrome, managed with diet and exercise, and her family history includes type 2 diabetes mellitus (mother and older sister). Laufala’s body mass index (BMI) is estimated at 28 kg/m2. She reports lethargy, polydipsia and polyuria since confirming her pregnancy.
You confirm the pregnancy with a urine dipstick and perform a fingerprick blood glucose level (BGL), which reads 16.0 mmol/L. Her bedside blood ketone level is 0.1 mmol/L.
What are your main concerns for Laufala?
Answer: Laufala presents with symptomatic hyperglycaemia. This is concerning and requires urgent treatment in the context of confirmed pregnancy. The fetus is vulnerable to the dangers of hyperglycaemia in early pregnancy and the mother may already have unrecognised hazardous microvascular complications. Intensive management to achieve target BGLs is needed to prevent or mitigate these risks.
You contact the endocrinologist on call at the nearest hospital and are advised to send Laufala to the Emergency Department. She is admitted to hospital for further assessment and management. Venous blood gas measurement shows normal pH and other biochemical parameters. Her formal blood glucose measurement is 15.6 mmol/L; HbA1c level is 8.0% (64 mmol/mol); fasting C-peptide level is high; and autoantibodies for type 1 diabetes (including glutamic acid decarboxylase [GAD], insulinoma associated antigen-2 [IA-2] and zinc transporter isoform 8 [Zn-T8] autoantibodies) are negative.
What is the likely diagnosis in this case?
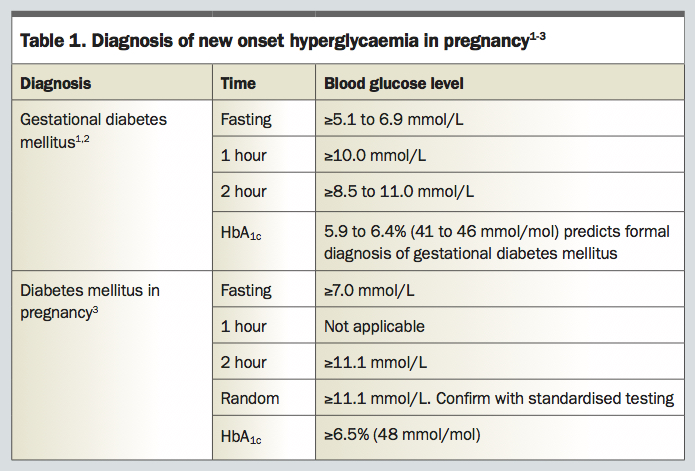
Answer: Hyperglycaemia that is first detected during pregnancy can be classified as either diabetes mellitus in pregnancy or gestational diabetes mellitus (GDM).
1-3 Laufala’s HbA
1c level is 8.0% (64 mmol/mol) and this meets the WHO criteria for diabetes mellitus in pregnancy (
Table 11-3). Diabetes mellitus in pregnancy often reflects unrecognised pre-existing diabetes, and the negative test results for type 1 autoantibodies are strongly suggestive of type 2 diabetes. However, a definitive diagnosis cannot be established during pregnancy and postpartum reassessment regarding the diagnosis is required.
Early recognition of women at risk of diabetes mellitus in pregnancy is an important aspect of management in the general practice setting. Routine screening for GDM occurs at 24 to 28 weeks’ gestation in the form of a 75 g oral glucose tolerance test (OGTT). However, those at high risk of developing diabetes (Box 1) and those who have overt symptoms of hyperglycaemia such as Laufala should have an early diagnostic test for diabetes at the earliest opportunity in pregnancy, ideally at confirmation of pregnancy.
A multiple daily insulin regimen consisting of insulin aspart before meals and twice-daily isophane insulin (NPH) is initiated for Laufala. Diabetes education, including input from a dietitian, is facilitated during her admission. Follow up in the multidisciplinary specialist antenatal clinic is arranged at discharge for the following week.
What are the principles of blood glucose management in women with diabetes mellitus in pregnancy?
Answer: Diabetes mellitus in pregnancy is managed similarly to pregestational diabetes (i.e. type 1 or type 2 diabetes diagnosed before pregnancy). It requires increased surveillance and monitoring. Education on insulin therapy, glucose monitoring, diet, exercise and driving is given, preferably by clinicians with experience in managing pregnant women with diabetes. A multidisciplinary team approach is ideal for this purpose.
Insulin therapy is safe and the first choice of pharmacotherapy in diabetes mellitus in pregnancy. If BGLs are substantially elevated as in Laufala’s case, then insulin therapy must be initiated promptly. A multiple daily injection regimen is preferred. Rapid-acting insulin lispro and insulin aspart have minimal placental transfer and are not linked to congenital malformations (both are category A in pregnancy). Similarly, the intermediate-acting isophane insulin (NPH) and the long-acting insulin detemir have established safety and efficacy in pregnancy (both category A). Fewer data are available for insulin glargine (category B3) but evidence suggests no adverse effects in pregnancy.4 Note that insulin detemir is PBS subsidised only for use in type 1 diabetes.5
Self-monitoring of BGLs (SMBG) is necessary to achieve glycaemic targets. Ideally, patients should perform finger-prick tests preprandially, postprandially (one or two hours) and at bedtime. The Australasian Diabetes in Pregnancy Society has recommended BGL targets for pregnant women with pre-existing diabetes (Table 2).6
Ultimately, BGL targets should be individualised to be safe for the individual woman, aiming for glucose levels in the normal range and avoidance of hypoglycaemia. In pregnant women with type 1 diabetes, the use of continuous blood-glucose monitoring (CGM) in conjunction with SMBG has led to favourable neonatal outcomes by reducing exposure to maternal hyperglycaemia.7 CGM products are subsidised by the National Diabetes Services Scheme in Australia for pregnant women with type 1 diabetes. However, pregnant women with other types of diabetes are not covered and the cost of CGM is high.
Metformin has modest blood-glucose lowering effects and a lower rate of hypoglycaemia compared with insulin. Although it readily crosses the placenta and is a category C drug, it is not associated with teratogenicity.8 There is variability across Australia regarding clinician prescription of metformin because of the limited data regarding long-term effects on offspring. Recent evidence has linked metformin exposure in utero to children with higher BMI at 7 to 9 years of age.9 No other forms of oral or injectable antihyperglycaemic agents have documented safety in pregnancy and should be discontinued.10
The frequency of antenatal visits is dependent on BGL control and the presence of complicating factors such as macrosomia or pre-eclampsia. The typical antenatal schedule is four weekly until 32 weeks, two weekly until 36 weeks and then weekly until delivery.
Laufala has an ultrasound scan at twelve weeks’ gestation that confirms viability and gestational age of her baby. A second trimester morphology scan is performed at 20 weeks’ gestation and is normal.
What are the potential congenital abnormalities associated with diabetes mellitus in pregnancy?
Answer: Babies of women with diabetes mellitus in pregnancy are at higher risk of congenital abnormalities compared with the background population. These risks include anencephaly, microcephaly, neural tube defects and congenital heart disease, and they are directly proportional to the elevation in HbA1c level during the first trimester of pregnancy.11 This reinforces the importance of morphological ultrasound scans.
The first trimester scan, which is used to confirm viability and gestational age, can also act as an early anatomy scan as it can identify early anomalies such as neural tube defects. The 20-week morphology scan is the most detailed anatomical ultrasound scan. In-utero exposure to hyperglycaemia is associated with the development of metabolic disturbances (obesity, type 2 diabetes, hyperlipidaemia) in the offspring of the mother with diabetes. It is thought that epigenetic mechanisms may play a role.12
Laufala attends the antenatal clinic. The result of a spot urine test for albumin to creatinine ratio is normal. An ophthalmology assessment shows no evidence of diabetic retinopathy.
What microvascular complications of diabetes are aggravated during pregnancy?
Answer: Women with diabetes mellitus in pregnancy are at increased risk of microvascular complications such as diabetic retinopathy. Retinopathy can be aggravated by rapid changes in glycaemia and the pregnant state itself. The retina should be examined before conception and during each trimester. Proliferative retinopathy should be treated with panretinal photocoagulation at the time of diagnosis. Antivascular endothelial growth factor therapy should be avoided due to fetal safety concerns.13,14
Pregnancy can also worsen pre-existing diabetic nephropathy by increasing proteinuria and reducing the glomerular filtration rate. The presence of microalbuminuria or macroalbuminuria indicates greater risk of pre-eclampsia in pregnancy. Proteinuria should be screened for using a urine dipstick at regular intervals.6,13
Laufala’s BGLs begin to improve and she is feeling more energised. She is keen to make lifestyle changes.
What do you advise?
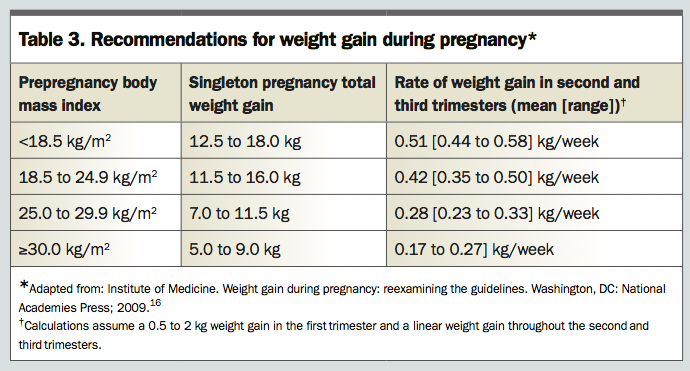
Answer: General advice regarding healthy lifestyle habits and optimal gestational weight gain should be provided. Women with diabetes mellitus in pregnancy should be referred to an accredited practising dietitian to provide individualised medical nutrition therapy.
15 The goals are to provide adequate nutritional intake for a healthy pregnancy, achieve target BGLs, prevent ketosis and maintain weight gain within recommended parameters (
Table 316). Exercise is beneficial. Half an hour of moderately intense physical activity several days of the week helps to minimise excessive weight gain and maintain glycaemic control.
17
Laufala’s insulin requirements begin to rise from week 18. Her endocrinologist explains that this is expected throughout the second and third trimester due to diabetogenic placental hormones increasing insulin resistance. Fortunately, Laufala’s HbA1c is 6.0% (42 mmol/mol) in the second trimester and 5.8% (40 mmol/mol) in the third trimester, reflecting improved insulin control. Her antenatal visits and fetal surveillance become more frequent. Laufala begins to worry about the safety of her pregnancy.
What are the potential obstetric complications for Laufala?
Answer: The increased risks to the pregnancy for women with diabetes include pre-eclampsia, miscarriage, premature delivery and stillbirth. Pre-eclampsia risk is multifactorial and related to midtrimester insulin resistance, pregestational hypertension and renal and vascular disease.18 The Royal Australian and New Zealand College of Obstetricians and Gynaecologists supports low-dose aspirin (100 mg per day taken at night time) and calcium supplementation for women with major pre eclampsia risk factors such as diabetes. Aspirin is initiated at 12 weeks’ gestation and discontinued at 36 weeks.19
From 28 to 36 weeks serial ultrasound scans are performed every four weeks to monitor fetal growth and amniotic fluid volume. The presence of large for gestational age (LGA) or intrauterine growth restriction increases the likelihood of complications at delivery, such as neonatal hypoglycaemia, birth trauma, shoulder dystocia and brachial plexus injury.18 Close monitoring and careful deliberation on the timing and type of delivery is warranted.
A growth scan at 32 weeks’ gestation shows an LGA neonate. Laufala continues attendance at the high-risk obstetric clinic for further birth planning.
What is the recommended approach to planning Laufala’s delivery?
Answer: It is recommended that women with diabetes mellitus in pregnancy give birth within a time frame similar to that recommended for women with pre-existing type 1 or type 2 diabetes. UK National Institute for Health and Care Excellence guidelines recommend that delivery occurs between 37 weeks and 38+6 weeks either by induction or planned caesarean section.9 The presence of high-risk features such as LGA, foetal growth restriction, worsening nephropathy or retinopathy, pre-eclampsia or uncontrolled dysglycaemia warrants consideration of an even earlier delivery. This should take place in a hospital where special care nursery facilities and advanced neonatal resuscitation skills are available.20
Steroids may be given for fetal lung maturation to women at risk of preterm birth; however, steroids can cause rapid worsening in glycaemic control and even precipitate diabetic ketoacidosis. Closely monitored insulin dose escalation, which sometimes requires hospital admission, is necessary for maintenance of euglycaemia.21
Laufala gives birth to a healthy boy by emergency caesarean section after failed induction of labour at 38+4 weeks’ gestation. The birthweight is 4050 g and BGLs in the first few hours of age are normal. Laufala’s postpartum laboratory fasting BGLs were between 5 and 6 mmol/L and therefore within normal range. She was discharged to your care.
A formal 75 g OGTT was arranged for 12 weeks postpartum. It confirms the diagnosis of type 2 diabetes mellitus and you initiate metformin therapy.
What is the postpartum management for women with diabetes mellitus in pregnancy?
Answer: After giving birth the diabetogenic actions of placental hormones diminish quickly and many women return to their prepregnancy glycaemic state. Given that a proportion of women with diabetes mellitus in pregnancy may have undiagnosed type 2 diabetes, it is vital to monitor BGLs in the first few days after the birth for evidence of persisting hyperglycaemia.
The presence of laboratory fasting BGLs greater than 7 mmol/L on two occasions is consistent with the diagnosis of diabetes. Continuation of medical nutrition therapy, physical activity and SMBG should be encouraged.22 Antihyperglycaemic agents can be considered and options safe for breastfeeding mothers include insulin, sulfonylureas and metformin.10,23 If fasting BGLs are less than 7 mmol/L, as in the case of Laufala, then it is recommended that a 75 g OGTT be performed at six to 12 weeks postpartum to ascertain the glycaemic status post pregnancy.21
Ophthalmological surveillance in the first year postpartum is recommended, as retinopathy can still be exacerbated within that time period. Retinopathy requiring laser therapy should be treated before subsequent pregnancies.6
Laufala returns to your medical centre. She is keen to have another child in the future.
What do you advise?
Answer: In the postpartum period for a woman with diabetes GPs should re-establish contact early with the mother and child for continuation of care. Future pregnancies should be planned, contraception encouraged and preconception counselling provided. This includes cessation of smoking, review of all medications for safety in pregnancy, screening for diabetic complications and commencement of high-dose folic acid supplementation. Education should be provided about the dangers of miscarriages and major congenital anomalies if hyper-glycaemia is not optimised before the next pregnancy. Contraception should be encouraged to avoid unintentional pregnancy before optimisation of glycaemia.
6 A preconception target HbA
1c of less than 6% (42 mmol/mol) is preferred provided it does not cause severe hypoglycaemia to the mother.
5 See
Box for helpful practice points.
COMPETING INTERESTS: None.
References
2. Nankervis A, Price S, Conn J. Gestational diabetes mellitus: a pragmatic approach to diagnosis and management. AJGP 2018; 47: 445.
4. O’Neill SM, Kenny LC, Khashan AS, West HM, Smyth RM, Kearney PM. Different insulin types and regimens for pregnant women with pre-existing diabetes. Cochrane Database Syst Rev 2017; (2): CD011880.
5. Gunton JE, Cheung NW, Davis TM, Zoungas S, Colagiuri S. A new blood glucose management algorithm for type 2 diabetes: a position statement of the Australian Diabetes Society. Med J Aust 2014; 201: 650-653.
6. McElduff A, Cheung NW, McIntyre HD, et al. The Australasian Diabetes in Pregnancy Society consensus guidelines for the management of type 1 and type 2 diabetes in relation to pregnancy. Med J Aust 2005; 183: 373-377.
7. Feig DS, Donovan LE, Corcoy R, et al. Continuous glucose monitoring in pregnant women with type 1 diabetes (CONCEPTT): a multicentre international randomised controlled trial. Lancet 2017; 390: 2347-2359.
8. Rowan JA, Hague WM, Gao W, Battin MR, Moore MP. Metformin versus insulin for the treatment of gestational diabetes. N Engl J Med 2008; 358: 2003-2015.
9. Rowan JA, Rush EC, Plank LD, et al. Metformin in gestational diabetes: the offspring follow-up (MiG TOFU): body composition and metabolic outcomes at 7-9 years of age. BMJ Open Diabetes Res Care 2018; 6(1): e000456.
11. Guerin A, Nisenbaum R, Ray JG. Use of maternal GHb concentration to estimate the risk of congenital anomalies in the offspring of women with prepregnancy diabetes. Diabetes Care 2007; 30: 1920-1925.
12. Moen GH, Sommer C, Prasad RB, et al. Mechanisms in endocrinology: epigenetic modifications and gestational diabetes: a systematic review of published literature. Euro J Endocrinol 2017; 176: R247-R267.
13. Irfan S, Arain TM, Shaukat A, Shahid A. Effect of pregnancy on diabetic nephropathy and retinopathy. J Coll Physicians Surg Pak 2004; 14: 75-78.
14. Rosenthal JM, Johnson MW. Management of retinal diseases in pregnant patients. J Ophthalmic Vis Res 2018; 13: 62-65.
15. Kitzmiller JL, Block JM, Brown FM, et al. Managing pre-existing diabetes for pregnancy: summary of evidence and consensus recommendations for care. Diabetes Care 2008; 31: 1060-1079.
16. Institute of Medicine. Weight gain during pregnancy: reexamining the guidelines. Washington, DC: National Academies Press; 2009.
17. Harris GD, White RD. Diabetes management and exercise in pregnant patients with diabetes. Clin Diabetes 2005; 23: 165-168.
18. HAPO Study Cooperative Research Group, Metzger BE, Lowe LP, et al. Hyperglycemia and adverse pregnancy outcomes. N Engl J Med 2008; 358: 1991-2002.
20. Maso G, Piccoli M, Parolin S, Restaino S, Alberico S. Diabetes in pregnancy: timing and mode of delivery. Curr Diab Rep 2014; 14: 506.
21. Bedalov A, Balasubramanyam A. Glucocorticoid-induced ketoacidosis in gestational diabetes: sequela of the acute treatment of preterm labor: a case report. Diabetes Care 1997; 20: 922-924.
22. Kitzmiller JL, Dang-Kilduff L, Taslimi MM. Gestational diabetes after delivery: short-term management and long-term risks. Diabetes Care 2007; 30 Suppl 2: S225-S235.
23. Briggs GG, Ambrose PJ, Nageotte MP, Padilla G, Wan S. Excretion of metformin into breast milk and the effect on nursing infants. Obstet Gynecol 2005; 105: 1437-1441.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}