Diabetes caused by pancreatic dysfunction: what you need to know

Pancreatic diseases
Diabetes medicines
Chronic pancreatitis, pancreatic cancer and other pancreatic disorders can cause diabetes that may be insulin dependent. ‘Pancreatogenic’ diabetes underlies 2 to 10% of diabetes cases and has specific management implications, but is frequently misdiagnosed.
- Diabetes caused by pancreatic disease accounts for 2 to 10% of diabetes cases, and may be more common than type 1 diabetes.
- The most common underlying cause is acute or chronic pancreatitis. Other causes include pancreatic cancer, surgical pancreatectomy, haemochromatosis and cystic fibrosis.
- Clinical features that may raise suspicion for underlying pancreatic disease in a patient with diabetes include low/normal body weight or weight loss, negative type 1 diabetes antibodies and low serum C-peptide levels. Further tests such as faecal elastase level and abdominal imaging may assist diagnosis.
- Insulin is the best treatment. Patients may also benefit from pancreatic enzyme and fat-soluble vitamin supplementation.
The importance of the pancreas in diabetes was first discovered in the 1880s when researchers removed the pancreas from a dog and observed that the animal developed rapidly fatal diabetes. Diabetes affects around 1.2 million Australians, or 5.1% of the population.1 Doctors are familiar with type 1 and type 2 diabetes; however, diabetes caused by exocrine pancreatic disease, injury or surgery is under-recognised. So-called ‘type 3C’ or ‘pancreatogenic’ diabetes can range in severity from transient high blood glucose levels to total insulin dependence and is frequently misdiagnosed, even by specialists. Some studies suggest pancreatogenic diabetes is more common than type 1 diabetes, but that it is frequently mistaken for type 2 diabetes. It is important to recognise patients with pancreatogenic diabetes as they are more likely to require insulin early, may benefit from pancreatic digestive enzyme supplementation and may be at risk of diabetic ketoacidosis.
Diabetes classification
Elevated blood glucose levels occur due to either insulin resistance or reduced insulin production, or a combination of the two. The current WHO classification recognises a number of causes of diabetes (Box).2 Type 1 diabetes is caused by autoimmune destruction of insulin-producing beta islet cells, whereas type 2 diabetes is caused by systemic insulin resistance and subsequent pancreatic ‘burnout’ as insulin production is unable to meet demand.
{kind=link}
Disease or surgical removal of the pancreas also causes diabetes due to loss of insulin-making capacity. This was once classified as a subset of ‘type 3’ diabetes that included other less common causes, but this classification is no longer used.
Relationship between the endocrine and exocrine pancreas
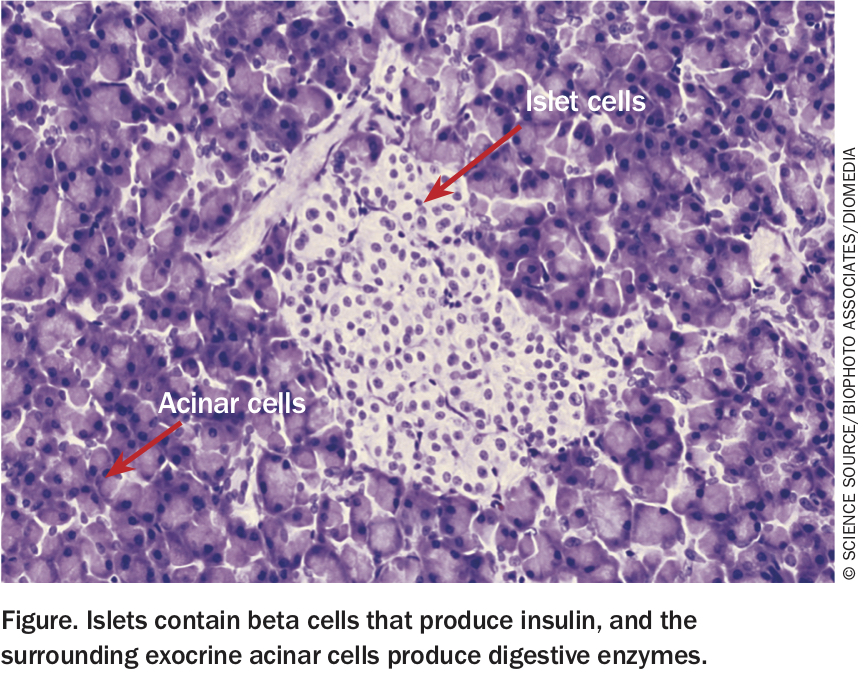
Endocrine islets account for 1 to 2% of total pancreatic mass and contain beta cells that produce insulin as well as other cells that produce regulatory hormones such as glucagon, somatostatin and pancreatic polypeptide (Figure).3 The surrounding exocrine acinar cells produce digestive enzymes (e.g. lipase, amylase, elastase and trypsinogen), which drain into the pancreatic ducts and then the gut. Paracrine signalling mediates communication between the exocrine and endocrine pancreas, so damage to the pancreas may lead to loss of both endocrine (diabetes) and exocrine (impaired digestion and malabsorption) function. This may occur suddenly in the context of surgery or acute severe pancreatitis, or develop more gradually in the context of inflammation and cytokine damage, as observed in chronic pancreatitis, cystic fibrosis-related diabetes and other disease processes.
{kind=link}
Causes of pancreatogenic diabetes
Any damage to the pancreas could lead to diabetes. This includes both acute and chronic pancreatitis, pancreatic cancer, surgical pancreatectomy, haemochromatosis (‘bronze’ diabetes, due to the associated skin pigmentation), cystic fibrosis-related damage, pancreatic trauma and congenital pancreatic agenesis.4
Pancreatitis is the most common cause and can be precipitated by alcohol, smoking, hypertriglyceridaemia, gallstones, hereditary mutations or autoimmunity (e.g. immunoglobulin G4 disease), or may be idiopathic.5 Typically, tissue damage must be extensive for pancreatitis to cause diabetes; however, even a relatively small pancreatic adenocarcinoma may be associated with diabetes through mechanisms that are unclear.
How common is diabetes due to pancreatic disease?
A number of studies have quantified the proportion of people with diabetes due to pancreatic disease. A German study from 2012 reviewed the records of almost 2000 patients with diabetes admitted to a specialist gastroenterology hospital and reclassified them as having type 1, type 2 or ‘type 3’ diabetes.6 The presence of ‘type 3’ pancreatic diabetes was established based on strict criteria including exocrine pancreatic insufficiency (faecal elastase level less than 200 mcg/g), imaging (CT or abdominal ultrasound) showing pancreatic abnormality and negative antibodies associated with type 1 diabetes. This study found that 9.2% of all patients with diabetes (172/1868) met the criteria for pancreatogenic diabetes. A significant number of these had been misclassified as having either type 1 (6.4%) or type 2 diabetes (40%) during their hospital stay.6 Chronic pancreatitis was the most common underlying cause, seen in 79% of cases. Other causes were pancreatic cancer (8%), hereditary haemochromatosis (7%), cystic fibrosis (4%) and pancreatic surgery (2%).6 Since this study was conducted at a gastroenterology centre, these rates of pancreatic disease may be an overestimate of population prevalence, but the proportion of patients with pancreatogenic diabetes was surprisingly high.
A nationwide study from New Zealand in 2017, based on a population database, analysed International Classification of Diseases-10 codes and found the population prevalence of pancreatogenic diabetes was 1.13/1000, similar to that of type 1 diabetes.7 The prevalence was highest in patients aged 70 to 79 years (3.94/1000) and in men (1.32/1000), and the prevalence in people of Maori and Pacific Islander ethnicity was three times that of people of European ethnicity.7
A further study from a UK primary care database showed that 1.8% of adult-onset diabetes followed pancreatic disease, which exceeded the incidence of type 1 diabetes. In this study, 88% of cases were misclassified as type 2 diabetes.8 In comparison with type 2 diabetes, however, patients with pancreatogenic diabetes had worse glycaemic control (odds ratio, 1.7) and were more likely to require insulin (40% vs 4% within five years). A review has estimated that pancreatogenic diabetes accounts for 5 to 10% of cases of diabetes in Western populations.5
Making the diagnosis
Currently, there are no formal guidelines or diagnostic criteria for diabetes associated with pancreatic disease. However, a number of clinical features may raise suspicion in a patient with newly diagnosed diabetes. These include a history of pancreatitis or other disorders associated with pancreatic dysfunction, low or normal body mass index, unexplained weight loss and/or abdominal pain, low serum C-peptide levels at the time of diagnosis (indicating impaired insulin production) and negative antibodies associated with type 1 diabetes. Abnormality on pancreatic imaging (CT/ultrasound) may also raise suspicion. Ketones may also be present.
Faecal elastase is the best available test to assess pancreatic exocrine function. A level less than 200 mcg/g is consistent with exocrine pancreatic dysfunction. Elevated serum lipase and amylase may be useful in diagnosing acute pancreatitis but are not accurate in assessing pancreatic function.
As a complicating factor, patients with longstanding type 1 and type 2 diabetes are more likely to have exocrine pancreatic failure than the general population due to pancreatitis and pancreatic cancer, which can lead to a ‘chicken or egg’ scenario.
Patients with a history of pancreatitis should be screened with annual fasting glucose and glycated haemoglobin tests, as should patients with cystic fibrosis and hereditary haemochromatosis.
Treatment of pancreatogenic diabetes
Because of the spectrum of severity, treatment needs will vary. The most severe cases – people with complete loss of pancreatic function – should be treated with basal-bolus insulin as for type 1 diabetes, keeping in mind that these patients may be at risk of ketoacidosis if treatment is interrupted. Even in less severe cases, insulin is the best treatment rather than oral hypoglycaemic agents, and the optimal insulin regimen will depend on the pattern of hyperglycaemia. Pancreatogenic diabetes may be associated with more ‘brittle’ glycaemic control due to loss of pancreatic counter-regulatory hormones (e.g. glucagon) and increased insulin sensitivity. Patients scheduled to have surgical pancreatectomy (e.g. Whipple procedure) should receive preoperative counselling and diabetes educator review, as learning to manage insulin-dependent diabetes will be an important part of their postoperative recovery.
Patients will likely have concurrent exocrine pancreatic enzyme deficiency and may be at risk of malnutrition, malabsorption, weight loss and nutritional deficiency, particularly of fat-soluble vitamins (A, D, E and K). Impaired fat digestion negatively impacts the incretin response, which may further worsen hyperglycaemia.3,4 Patients therefore benefit from taking pancreatic enzyme supplements.
Conclusion
Depending on the clinical setting, 2 to 10% of diabetes cases are caused by diseases affecting the exocrine pancreas, but pancreatogenic diabetes is frequently misdiagnosed. Pancreatitis is the most common cause. Suggestive clinical features include history of pancreatic disease, patients with low/normal body mass index, low serum C-peptide levels and pancreatic abnormalities on imaging. A low faecal elastase level may confirm exocrine pancreatic failure. Insulin is the treatment of choice, and prompt initiation can avoid complications including potential diabetic ketoacidosis. Many patients will also benefit from pancreatic enzyme and fat-soluble vitamin supplementation. ET