Vertebral fracture in a 60-year-old woman

Fractures
Back pain
The immediate management and investigation of an acute endocrine presentation in general practice is discussed in this section. It is inspired by, but not based on, a real patient situation.
Lily, a 60-year-old shop assistant, presents with sudden onset of back pain after bending down to pick up a tray of mangoes at work. The pain is located in the mid-back and has not resolved after 48 hours of bed rest. On examination, she has acute tenderness in the midline, at the lower thoracic level. She is afebrile, has no systemic symptoms and neurological examination is normal.
What is the differential diagnosis of acute back pain?
Answer: Acute back pain is one of the most common adult presentations in general practice. It may be categorised according to causes that are:
1. Intrinsic. Intrinsic spine conditions include vertebral compression fractures, disc herniation, lumbar strain/sprain, spinal stenosis, spondylolisthesis and degenerative disc or facet joint arthropathy. These occur commonly and are characterised by pain exacerbated by movement.
2. Systemic. Back pain related to systemic disease tends to be nonmechanical, often present at night or continuously, and accompanied by systemic features such as fever, weight loss or other joint involvement. Causes include connective tissue disease, inflammatory spondyloarthropathies, malignancy or vertebral discitis/osteomyelitis.
3. Referred. Referred pain from visceral disease should also be considered, including aortic aneurysm; gastrointestinal, retroperitoneal or pelvic organ inflammation; renal colic or herpes zoster.
Certain red flags alert the GP to more sinister pathologies that require further investigation. These include neurological features (incontinence, motor or sensory loss), history of traumatic injury, fever, immunosuppression, glucocorticoid use and risk factors for osteoporosis. Many red flags are not specific – 80% of patients presenting in primary care may have at least one red flag, but most of these will not have serious pathology.1 Good clinical judgement, and taking the whole patient and scenario into consideration is more important than the number of red flags.
Lily migrated to Australia five years ago and lives with her adult daughter and grandchildren. She is an active woman who has worked in physical jobs all her life and also cares for her three grandchildren. She has a past history of treated Graves’ disease in her twenties, but is otherwise healthy and on no regular medication. She has not had previous episodes of back pain or clinical fracture. She has not had any falls. She is a lifelong nonsmoker and nondrinker. She is 152 cm tall and weighs 45 kg.
You suspect that Lily has sustained a vertebral crush fracture and order a thoraco-lumbar spine x-ray. The x-ray reveals a 30% reduction in vertebral height at T12. All other vertebral bodies are preserved.
How should acute vertebral crush fractures be managed?
Answer: Management of vertebral crush fractures is guided by history and clinical examination findings. Neurological deficits, bladder or bowel dysfunction, or saddle anaesthesia may indicate retropulsed bone fragments in the spinal canal or foramina, requiring urgent surgical intervention. Surgery should also be considered when multiple vertebrae are involved, as these fractures tend to be unstable. Otherwise, management of vertebral fractures is largely targeted at analgesic control. Begin with nonopioid medication such as paracetamol or nonsteroidal anti-inflammatory drugs for mild pain. Add opioids if the pain is severe or inadequately controlled with initial medication. Early mobilisation after 24 to 48 hours of rest is encouraged and a brace may be used acutely to minimise pain, if required. Prolonged use of a brace is not recommended due to atrophy of core muscles and promotion of further bone loss.
Vertebral augmentation may be considered in patients with persistent pain. Vertebroplasty and kyphoplasty involve percutaneous injection of bone cement into a fractured vertebra under image guidance, acting as an internal splint to reinforce and stabilise the fracture for pain alleviation. Kyphoplasty is more technically challenging than vertebroplasty, as it involves a bilateral catheter approach – a balloon is inflated to create a cavity into which cement is injected.2 Multiple meta-analyses have shown no significant differences in short- or long-term pain scores or disability scores between the two procedures. In fact, a recent analysis of five sham-procedure randomised placebo-controlled trials reported no demonstrable benefit of vertebroplasty in patients with acutely painful vertebral fracture compared to placebo.3 However, one randomised study using vertebroplasty soon after fracture showed acute benefit.1,2
There is a current lack of consensus regarding the role of vertebroplasty, but some experts would consider its use in patients with incapacitating pain who are not improving after four weeks, or who are intolerant to analgesics.4 Benefits may include improvements in pain and functional capability, and limiting height loss. Complications include extravasation of cement causing increased pain, damage to the spinal cord or nerve roots, infection and local acceleration of bone resorption, and fractures of adjacent vertebrae related to the treatment itself (although this was not proven in the current review) or to a foreign body reaction.
Lily’s pain gradually resolves with simple analgesia and she resumes general mobility. Lily is concerned about why the fracture occurred in the course of her usual activity and if she is at risk of recurrence. You deem that Lily has sustained a minimal trauma fracture and that further investigation is necessary.
What is the definition of a minimal trauma fracture?
Answer: Fractures occurring in the absence of major trauma, i.e. without any obvious initiating trauma or with minimal external trauma such as from a fall from standing height or less, are termed minimal trauma or fragility fractures. Minimal trauma fractures are a warning sign of poor bone health and should be further investigated.
Vertebral compression fractures are one of the most common types of fragility fracture. They may occur in the absence of trauma, or after only minor trauma such as bending, coughing or lifting. Most commonly, in about 70% of cases, they may be asymptomatic and found incidentally on radiographs of the chest or abdomen, but they occasionally present with signs of kyphosis, height loss or back pain. If not investigated and appropriately treated, individuals who sustain a vertebral fracture are two to four times more likely to sustain another vertebral fracture than other individuals of the same sex and age.
There is evidence that patients who experience fractures under moderate trauma, known as ‘more than minimal trauma’, may also have underlying osteoporosis. Such a mechanism of injury may, for example, be a fracture after a fall from slightly greater than standing height (such as falling from a stool) or a low-speed motor vehicle accident. This may be particularly relevant in post-menopausal women and older men, and a bone mineral density (BMD) scan is warranted in these situations (although it is not PBS-rebated).
How is the diagnosis of osteoporosis made?
Answer: Osteoporosis results from reduced density and quality of bone leading to increased bone fragility. It may be defined by either clinical or bone density criteria. A patient aged over 50 years experiencing a minimal-trauma fracture has a clinical diagnosis of osteoporosis, particularly if the fracture is at a typical site such as the hip, vertebra or wrist.
In order to identify patients at increased risk of bone fragility, even before a fracture occurs, the World Health Organization (WHO) have an operational definition of osteoporosis based on bone mineral density (Box).5
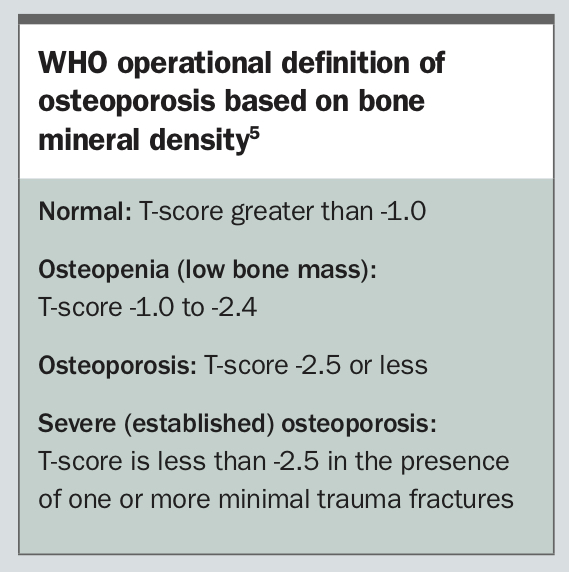{kind=link}
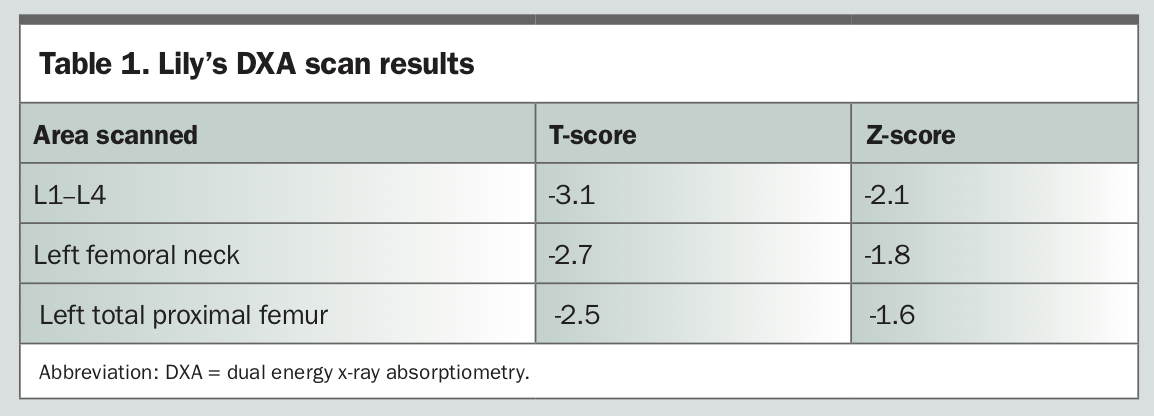
Lily has a dual energy x-ray absorptiometry (DXA) bone density
scan (Table 1).
{kind=link}
How should the T-score and Z-score be interpreted?
Answer: The T-score represents the number of standard deviations away from the healthy young adult mean. As expected, Lily has T-scores in the osteoporotic range, confirming her diagnosis of osteoporosis, both on clinical and radiographic grounds. The Z-score represents the number of standard deviations away from the mean of healthy people of the same age (and weight for some machines). Many older people will have low T-scores because of normal ageing alone; however, Z-scores of greater than -2.0 suggest low bone density relative to age, which should prompt investigation for a secondary cause of osteoporosis.
It is important to establish the baseline severity of osteoporosis with a bone density scan, which may impact on clinical decision-making, the need for further investigations for a secondary cause of osteoporosis, and the choice of osteoporosis therapy. Changes in bone density over time can be used to monitor response to treatment.
What is the role of DXA scanning in the assessment of bone density? How does quantitative CT differ?
Answer: DXA offers an established and accurate measure of bone mineral density and correlates with an individual’s risk of minimal trauma fracture. It involves a low dose of radiation and short scan time, and provides high reproducibility, which enables measurement of therapeutic response. There are different DXA systems (e.g. Lunar, Hologic, Norland) that use different technologies and different reference populations for T-score calculation. Serial DXA scans should be performed using the same system and, ideally, the same instrument, to allow accurate comparison. Bone density is best measured at the hip and lumbar spine. Changes in these sites have been demonstrated in response to osteoporosis treatment and correlate with a person’s subsequent fracture risk. Wrist BMD tends to be less reliable and is usually only done when hip and/or spinal sites cannot be assessed. It is not used to diagnose osteoporosis.
In addition to central DXA systems for measuring bone density at the spine and hip, other types of bone densitometry measurements are available. These include quantitative computed tomography (QCT) measurements of the spine and hip and peripheral DXA (pDXA) systems for measuring the forearm, heel or hand. These alternative types of measurement correlate poorly with DXA, involve a greater degree of radiation (particularly QCT) and have poorer reproducibility. Hence, there is lack of consensus regarding the use of these other methods.
What factors contribute towards low bone density? What further investigations are appropriate?
Answer: Nonmodifiable contributors to low bone density include genetic tendency and early age of menopause. Certain medical conditions and medications reduce bone density and quality, including rheumatoid arthritis, hypogonadism, hyperparathyroidism, hyperthyroidism coeliac disease/malabsorption, multiple myeloma, chronic liver disease, chronic renal failure, glucocorticoids and antiepileptic medication. Smoking, excessive alcohol use, low dietary calcium, vitamin D deficiency and lack of weight-bearing activity are important potentially modifiable factors, albeit with modest effect. Conduct a thorough history and examination, followed by selected investigations for secondary causes, based on clinical likelihood.
Lily grew up in Vietnam and describes a lifelong low calcium diet. She avoids direct sun exposure to protect her skin and does not take any vitamin supplements. She had three children in her twenties and breastfed for about five years. Her periods stopped at the age of 32 years, but she did not seek medical attention at the time and has not been on menopausal hormone therapy. She is not aware of a family history of fracture. She has never been on glucocorticoid therapy.
What is the role of oestrogen in bone protection? How should the bone health of women with premature menopause be managed?
Answer: Oestrogen plays an important role in the growth and maturation of bone and is required for proper closure of epiphyseal growth plates in women and men. In adult bone, oestrogen regulates bone turnover. Oestrogen deficiency results in increased osteoclast formation and promotes bone resorption, leading to net loss of both trabecular and cortical bone. Women who have experienced premature menopause, either naturally or surgically, are thus at increased risk of osteoporosis, and the use of oestrogen-containing menopausal hormone therapy (MHT) to protect against premature bone loss is important. Younger women may prefer to take oestrogen in the form of the oral contraceptive pill. MHT should continue at least until the natural age of menopause (50 to 54 years). Arguments about the risks of MHT in women beyond the average age of natural menopause are not relevant to this situation and MHT should be considered the standard of care unless there are specific contraindications. As Lily is now well past the natural age of menopause and has had a fracture, MHT would no longer be a first-line treatment option in her case.
In patients with an intact uterus, endometrial protection with progesteronic compounds is necessary. Combined transdermal oestrogen- progesterone formulations are available, or the progesterone may be administered locally via an intrauterine device or orally (such as with the use of micronised or synthetic progesterone formulations).
Blood tests reveal Lily has a low vitamin D level of 35 nmol/L and an appropriately elevated parathyroid hormone level of 15 pmol/L. Her calcium and phosphate levels are within normal ranges. She has normal renal function, liver function, thyroid function and full blood count test results. Her coeliac serological testing and myeloma screening results are negative.
You recommend that Lily increase her intake of calcium-rich foods, including bony fish (sardines), firm tofu (set with calcium) and calcium-fortified soy milk, which Lily finds more palatable than dairy. After discussing the different options for vitamin D replacement and ascertaining Lily’s preference, you commence her on once weekly vitamin D tablets (2 x 7000 IU tablets per week), with a plan to review the dose in three months.
How can fracture risk be estimated and utilised for clinical decision-making?
Answer: There is a clear inverse relationship between bone density and fracture. For every unit increase in BMD T-score, the risk of fracture decreases by 40%.6 However, many other factors contribute to fracture risk beyond bone density and should be included in the risk assessment and subsequent decision to commence antiresorptive therapy. In particular, a prior history of minimal trauma fracture, especially recent fracture, is a strong predictor of future fractures. Fracture risk calculators have been developed to assist clinicians in estimating a person’s five- and/or 10-year probability of fragility fracture and hip fracture based on multiple clinical factors, and can be used with or without a known BMD measurement. The Garvan Fracture Risk Calculator is a freely available web-based tool developed from a specifically Australian population that allows estimation of both five- and 10-year probability of hip fracture and any osteoporotic fracture.7 The Fracture Risk Assessment Tool (FRAX®) is also a freely available web-based and desk-top application that allows calculation of a person’s 10-year probability of hip fracture and major osteoporotic fracture (clinical spine, forearm, hip or shoulder), specific to their country/region of origin.8 The two tools utilise different clinical information and have their individual limitations, but both have been validated in various international cohorts for treatment-naïve patients.
There is debate about how absolute fracture risk results should be used to guide initiation of therapy. The Osteoporosis Australia/ RACGP guidelines recommend treatment with anti-osteoporosis medication for all individuals with minimal trauma hip or vertebral fractures and those with minimal trauma fractures at other sites who have T-scores of -1.5 or less. Individuals with T-scores -1.5 or more may still warrant consideration for treatment after specialist review. For individuals with no history of minimal trauma fracture, treatment is recommended for those aged 70 years and above who have T-scores of -2.5 or less, or those who have a 10-year risk of hip fracture above 3%, or any fracture above 20%.
The British National Osteoporosis Guideline Group (NOGG) 2017 guideline suggests treatment based on a prior fragility fracture (especially hip or vertebral) or the 10-year probability of major osteoporotic fracture, using an intervention threshold that increases with age up until age 70, then plateaus at 20% (Figure).9 However, the NOGG guidelines are based on cost–benefit analysis and may not reflect clinical benefit to an individual. In patients with a prior fracture, the risk of refracture is highest in the few years following the initial fracture.10 Thus, a 10-year fracture risk may not give a reliable picture of imminent fracture risk, particularly in older patients, and intervention might be considered even at lower thresholds, depending on the clinical situation.
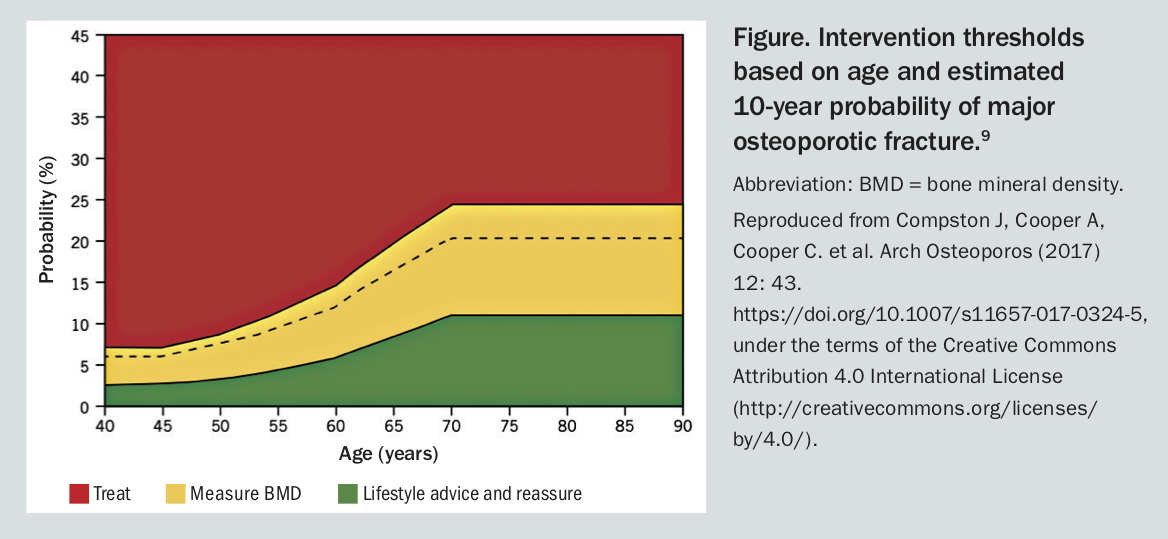{kind=link}
The recommendations from these guidelines are only partially reflected in the Australian PBS subsidy for antiresorptive agents, which is available to:
- all people with prior history of minimal trauma fracture (established osteoporosis)
- those aged 70 years and above with T-score of -2.5 or less
- individuals treated with supraphysiological glucocorticoid doses for at least three months with T-score of -1.5 or less.
The PBS subsidy does not apply to individuals with a high estimated 10-year risk of fracture unless the above clinical and BMD criteria are met. As the cost of generic bisphosphonates is low, the use of these medications on private prescription should be discussed with patients who meet guideline recommendations but not PBS criteria.
Given that Lily has had a vertebral fracture after minimal trauma, you determine that she is at high risk of a subsequent fracture and that antiresorptive therapy should be initiated.
What are the options for antiresorptive therapy and the risks and benefits of each treatment in Lily’s case?
Answer: Options for antiresorptive therapy include oral and IV bisphosphonates and subcutaneous denosumab injections. Therapy reduces the risk of subsequent fracture by 30 to 50%. In Australia, the PBS allows use of any of these agents in patients with a prior minimal trauma fracture. Choice of agent should incorporate both patient preference and individual clinical factors (Table 2).
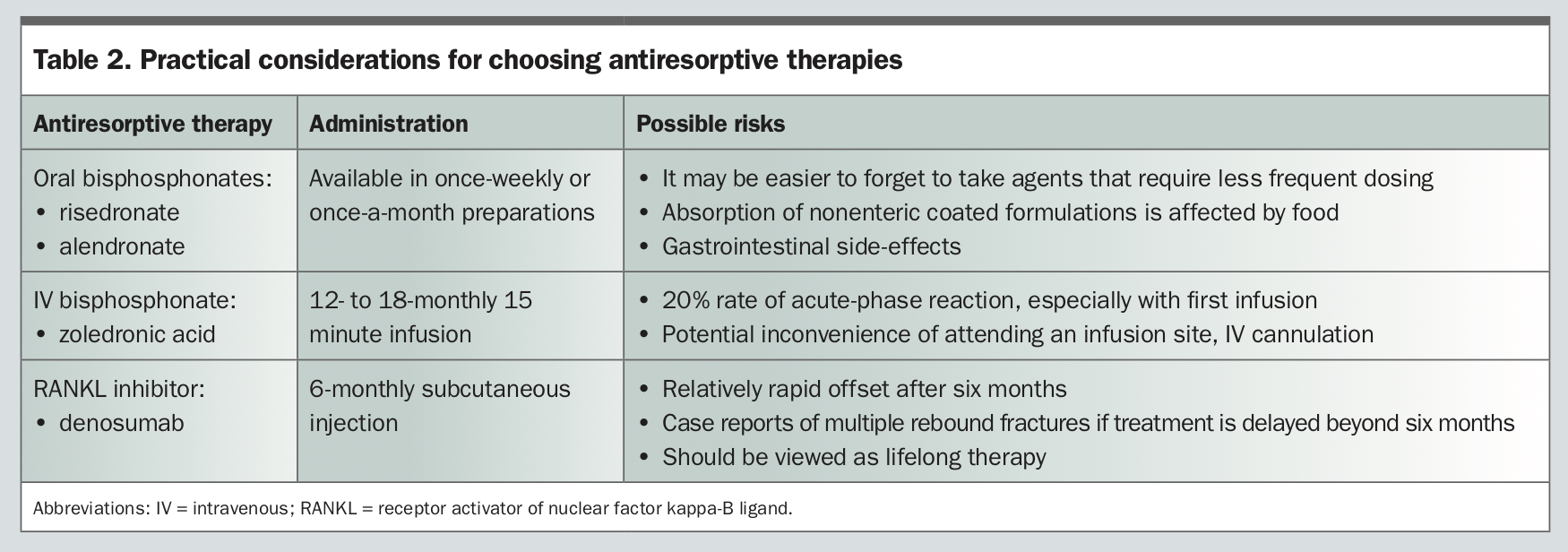{kind=link}
Both bisphosphonates and denosumab may precipitate hypocalcaemia, especially in patients with renal impairment and/or vitamin D deficiency. Vitamin D levels should be checked and rendered replete before administration. There is seasonal variation in vitamin D levels, which tend to drop after the winter months, even in people replete during summer. A recent measurement is always advisable. In those without risk factors, routine calcium monitoring is not required; however, in those on denosumab with estimated glomerular filtration rate of less than 30 mL/min, serum calcium should be checked seven to 10 days post-dose.
All antiresorptive agents carry a risk of rare long-term complications, including osteonecrosis of the jaw and atypical femoral fracture.11 These complications appear to increase with longer duration of therapy, especially beyond eight to 10 years, and may be attenuated by limited periods of drug withdrawal of one to two years (only in the case of bisphosphonates). Unfortunately, this exposes the patient to an increased risk of fragility fracture and the risk:benefit ratio of so-called ‘drug holidays’ remains contentious. The long-term risk of atypical femoral fracture may be an argument against commencing denosumab in a very young patient, who is then committed to potential decades of treatment – this is much debated. Importantly, in the setting of prior fragility fracture and high risk of refracture, patients should be clearly informed that the benefit of reducing subsequent fractures outweighs the small risks of these adverse events.
After discussion, Lily decides to proceed with an infusion of zoledronic acid, preferring the convenience of yearly administration over remembering a weekly or monthly tablet. To minimise the risk or severity of an infusion-related influenza-like reaction, she is advised to take regular paracetamol the day before, the day of, and day after her infusion.
Lily wants to know if she can return to her usual work, where she lifts weights of up to 5 kg while stacking shelves.
What advice on physical activity should be given to people with very low bone density?
Answer: Resuming physical activity is important after a fracture, as weight bearing provides mechanical loading to bones, which induces a physiological response that helps maintain bone strength. Additionally, strength and balance training may reduce the risk of falls. Safety is a prime consideration when returning to physical activity, as excessive forces or exercise-related falls might precipitate subsequent fractures. In the short term, Lily should resume gentle weight-bearing activities such as walking, tai chi, lunges, sideways stepping, step climbing and descent. She should avoid activities that involve repetitive jumping, bending and twisting (e.g. stacking shelves, carrying grandchildren). She should not lift weights greater than 4 to 5 kg. During lifting, she should keep her back straight and bend from the legs, keeping the weight close to the body and engaging her core by gently tensing and holding in her abdominal muscles, while maintaining normal breathing.
In consultation with a physiotherapist or exercise physiologist, progressive resistance training, especially involving muscle groups related to spine extension, hip abduction/extension and knee flexion/extension may be beneficial. In the longer term, research suggests that, if commenced at least one year after the fracture, a high intensity resistance and impact training program can be both safe and beneficial for bone density; however, this should be conducted in a highly supervised environment with trained personnel.12
Lily proceeds with an infusion of zoledronic acid and continues to take vitamin D on a regular basis as advised. You ask her to have a repeat bone density scan in 12 months to assess her initial response to this treatment and plan to give her another infusion in 12 months. ET