Endocrine causes of osteoporosis. Part 1: Primary hyperparathyroidism

Osteoporosis
Parathyroid disorders
Endocrine causes of osteoporosis, such as primary hyperparathyroidism, hypogonadism, glucocorticoid excess, acromegaly, Cushing’s syndrome and hyperthyroidism, are well-recognised risk factors for decreased bone mineral density. Optimal management of bone health in people with these conditions involves treating the underlying hormonal disease and assessing the need for specific bone preservation therapy. This three-part series discusses the management of three different cases to highlight the detrimental impact of specific endocrine disease on bone health.
- Elevated serum calcium and parathyroid hormone levels should raise the suspicion of underlying primary hyperparathyroidism.
- Measurement of bone mineral density at the lumbar spine, femoral neck and distal 1/3 radius using dual x-ray absorptiometry (DXA) is recommended in patients with primary hyperparathyroidism.
- Vitamin D replacement to a level above 50 nmol/L should be encouraged to reduce the potential risk of hungry bone syndrome after parathyroidectomy.
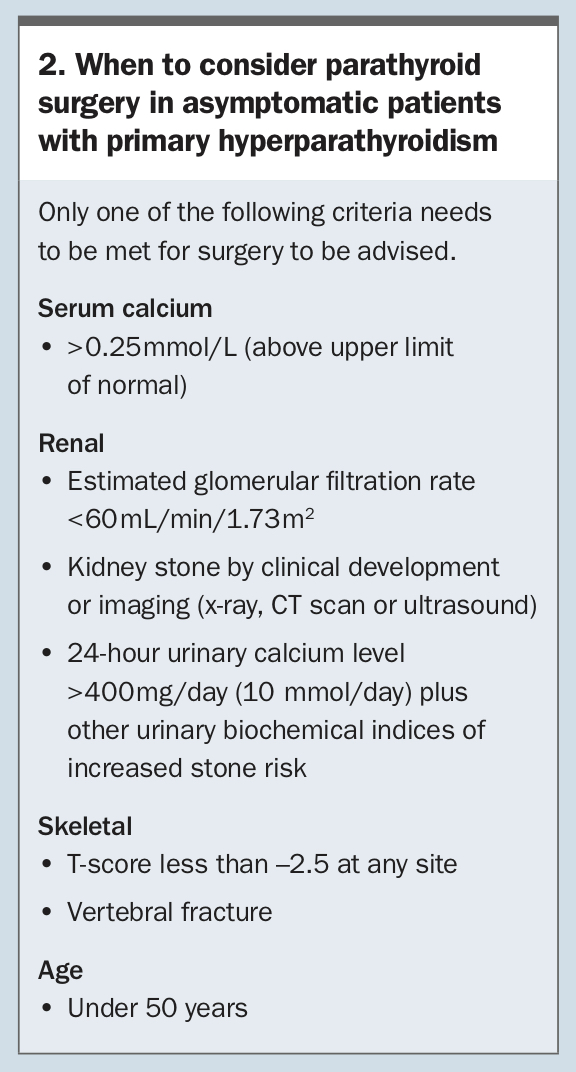
- Surgical resection is recommended for patients with symptomatic primary hyperparathyroidism and for asymptomatic patients who have a calcium level greater than 0.25 mmol/L above the upper limit of normal, renal impairment, nephrolithiasis or skeletal involvement (minimal trauma fracture or osteoporosis confirmed by DXA) or are under 50 years of age.
- A parathyroid Sestamibi and neck ultrasound should only be undertaken if a decision to proceed to surgery is made. A referral of the patient to an endocrinologist may be appropriate in these cases.
Osteoporosis is a recognised public health issue and GPs are at the front line in managing this disease. More than 4.74 million people over the age of 50 years in Australia have osteoporosis, osteopenia or poor bone health.1 Up to 30% of postmenopausal women and 50% of men with osteoporosis have a secondary cause.2 Osteoporosis in premenopausal women and young men (aged less than 50 years) is less common, and in this cohort investigating for a secondary cause for bone loss is important. There are multiple endocrine conditions that can accelerate bone loss (Box 1). Nonendocrine causes of osteoporosis include bone marrow-related disorders, chronic neurological disease associated with marked immobility, rheumatoid arthritis and transplant recipients.3,4
{kind=link}
Osteoporosis is more often than not identified through measurement of bone mineral density (BMD) by dual x-ray absorptiometry (DXA) and would otherwise be unidentified until time of fracture. Assessment of bone health in patients with relevant chronic endocrine diseases will facilitate timely intervention to prevent significant morbidity secondary to disabling fractures.
This three-part series highlights the detrimental impact of specific endocrine diseases on bone health. Part 1 discusses the management of primary hyperparathyroidism in an elderly woman, part 2 discusses glucocorticoid-induced bone loss in a 65-year-old man and part 3 discusses reduced BMD in a woman with premature ovarian insufficiency.
Primary hyperparathyroidism
Case scenario
Mrs Smith, a 75-year-old woman, was reviewed by her GP following minimal trauma fractures to her radius and ulna. Her DXA scan results were consistent with severe osteoporosis. Her lumbar spine (L1–L4) T-score was –4.2 and her right femoral neck T-score was –3.9. Her past history included hypertension and hysterectomy (ovaries preserved) at age 34 years. Her age of menopause was not known and she had never been on menopausal hormone therapy.
A secondary screen for osteoporosis revealed hypercalcaemia (corrected calcium level, 3.07 mmol/L; normal, 2.10–2.60 mmol/L) with an elevated parathyroid hormone (PTH) level (27.9 pmol/L; normal, 1.5–7.0 pmol/L), suggestive of primary hyperparathyroidism. Mrs Smith’s serum protein electrophoresis, free light chain levels, thyroid function tests, coeliac serology and vitamin D level (64 nmol/L) were normal. However, given the degree of hypercalcaemia, Mrs Smith was advised to present to the nearest emergency department.
Further investigations as an inpatient confirmed a corrected calcium level of 3.08 mmol/L (normal, 2.20–2.65 mmol/L), ionised calcium level 1.65 mmol/L (normal, 1.24–1.37 mmol/L), phosphate level 0.65 mmol/L (normal, 0.75–1.50 mmol/L) and PTH level 29 pmol/L (normal, 1.6–6.7 pmol/L). Her renal function was normal with estimated glomerular filtration rate of 83 mL/min/1.73m2. She had no history or symptoms consistent with nephrolithiasis. A formal diagnosis of primary hyperparathyroidism was made on the basis of these investigations.
She was admitted under the endocrinology unit and was initially treated with intravenous fluids. However, her corrected calcium level remained persistently above 2.90 mmol/L and she was referred to the endocrine surgeon for consideration of parathyroidectomy. A parathyroid Sestamibi scan and neck ultrasound were performed but failed to localise a parathyroid adenoma. After discussion with Mrs Smith, a bilateral neck exploration was performed. Two inferior parathyroid glands were identified as abnormal and removed. The other two glands were preserved. Calcium levels normalised the day after surgery to 2.45 mmol/L with a PTH level of 0.8 pmol/L. Two months later, her corrected calcium level was stable at 2.42 mmol/L with a PTH level of 2.7 pmol/L. Due to her history of minimal trauma fracture and the severity of her osteoporosis on DXA, Mrs Smith was also treated with intravenous zoledronic acid before discharge.
Discussion
Primary hyperparathyroidism is common in the community, generally presenting in people over the age of 50 years. It has a reported prevalence of 233 per 100,000 in women and 85 per 100,000 in men.5
Primary hyperparathyroidism is typically sporadic but when the diagnosis is made in younger patients (less than 40 years of age), genetic syndromes such as multiple endocrine neoplasia type 1 and 2A should be suspected. The typical biochemical presentation of primary hyperparathyroidism is an elevated serum corrected and/or ionised calcium level and elevated or unsuppressed PTH level. A corrected calcium level of more than 3 mmol/L is a reasonable threshold for referral of the patient to the emergency department for management and intervention. It is also worth discussing with an endocrinologist about the need for urgent investigation and management for patients with a corrected calcium level below 3 mmol/L who have rapid increases in corrected calcium levels despite adequate hydration.
The biochemical confirmation of primary hyperparathyroidism is paramount and must be distinguished from other causes of an elevated PTH level, such as vitamin D deficiency, poor dietary calcium intake and renal impairment, which are often seen in the primary care setting. Most patients do not present with any symptoms; however, a history of kidney stones or minimal trauma fracture should raise the clinical suspicion of primary hyperparathyroidism.
Excessive parathyroid hormone levels stimulate osteoclasts and lead to increased bone resorption. Sites that are rich in cortical bone, such as the femoral neck and distal 1/3 radius, are more severely affected in patients with primary hyperparathyroidism, but both vertebral and nonvertebral fracture risk is increased.6 Hypercalcaemia leads to increased glomerular filtration and hypercalciuria despite the actions of PTH to promote calcium absorption at the kidney tubules. Hypercalciuria promotes the formation of kidney stones.
Once primary hyperparathyroidism is confirmed on biochemistry, this should be followed by a focused history and examination of the potential associated end-organ complications. Consideration for a DXA study, 24-hour urine calcium excretion study and renal tract ultrasound to investigate for osteoporosis and asymptomatic nephrolithiasis are often appropriate. A parathyroid Sestamibi and neck ultrasound should only be undertaken if a parathyroidectomy is to be considered if an adenoma was identified.
The decision to undertake a parathyroidectomy will be influenced by the severity of hypercalcaemia and the patient’s general health and surgical risk. In general, patients younger than 50 years should be offered the chance of definitive cure with surgery. The indications for surgery in an asymptomatic patient include a calcium level greater than 0.25 mmol/L above baseline, the presence of osteoporosis on DXA criteria, minimal trauma fracture, kidney stone or impaired renal function (see Box 2).7
{kind=link}
Definitive treatment with parathyroidectomy can partially reverse the loss in BMD with reports of up to 15% increase in BMD in the first 12 months and up to 20% increase in BMD four years after successful parathyroidectomy.8 Parathyroidectomy is also associated with reduced fracture risk.
Vitamin D replacement to a level above 50 nmol/L should be encouraged after parathyroidectomy to reduce the potential risk of hungry bone syndrome. Hungry bone syndrome refers to prolonged hypocalcaemia, hypophosphataemia and hypomagnesaemia in the immediate postoperative period and is due to the reduction in PTH level.
In patients who are unsuitable for surgical treatment and have osteoporosis, antiresorptive therapy with a bisphosphonate will reduce the degree of hypercalcaemia and improve BMD. Alendronate has well-established efficacy in improving BMD in people with primary hyperparathyroidism.9 However, treatment with any oral or intravenous bisphosphonate is also effective.7 The dosing frequency for intravenous bisphosphonate therapy for patients with osteoporosis will be guided by their fracture risk, which will be influenced by factors including their surgical status (pre- or postparathyroidectomy), renal function, bone turnover markers, BMD, falls risk and incident fractures. Cinacalcet, a calcimimetic that acts by increasing the sensitivity of the calcium-sensing receptors on parathyroid glands to extracellular calcium, has proven benefits in attenuating hypercalcaemia in people with primary hyperparathyroidism, although it does not improve BMD.7 However, it is not currently listed on the PBS for the indication of primary hyperparathyroidism. ET